










 311 / 460
311 / 460

E. Gancel, R.A. Magnussen, F. Trouillet, S. Lustig, E. Servien, P. Neyret
310
Complications
Any early complication was observed. At last
follow-up, any revision was required and any
loosening was observed on radiography.
Discussion
This study is a medium-term retrospective
analysis of the results of eleven patients in
whom simultaneous UKA and partial lateral
patellar facetectomy was performed for
degenerative disease limited to one tibiofemoral
compartment and the lateral patellofemoral
joint. Our results indicate that this treatment
strategy is viable option for these patients as
good pain control and functional outcome were
achieved.
Although some UKA femoral component
designs have been noted to impinge of the
patella in some cases [15], this complication is
relatively rare and several authors have
demonstrated no significant differences in
patellofemoral joint forces and kinematics
following UKA [28, 32]. This finding suggests
that treatment strategies for patellofemoral
joint pathology, such as partial lateral
facetectomy, that are successful in patients with
isolated patellofemoral involvement will also
find success in patients that undergoing UKA.
The only previous results of the combination of
a non-arthroplasty procedure to treat patello
femoral arthritis with a UKA were reported by
Antoniou
et al
in 1996 [2]. They utilized the
patelloplasty technique described by Ficat
et
al.
[12] and Marmor [24] to resurface the entire
patella with fibrocartilage and noted relief of
patellofemoral pain in 90% of patients at six
years post-operative [2].
Other options are available for the treatment of
associated unicompartmental and patello
femoral degenerative disease.When the patello
femoral disease is asymptomatic, conservative
management of the patellofemoral joint has
been shown to be effective, with no adverse
effects on outcome of UKAnoted in this patient
population [5, 6, 7, 14]. When patellofemoral
disease is symptomatic, some authors have
reported good results through the combination
of patellofemoral arthroplasty and UKA [16].
More recently, specific bicompartmental
arthroplasty systems have been developed and
reported [33]. Palumbo reported poor results
for the bicompartmental arthroplasty [29]. Both
of these techniques have the theoretical
advantages of preserving both cruciate
ligaments and more normal gait [8, 9, 20].
Finally, TKA remains a standard technique for
the management of bicompartmental disease.
Patellofemoral joint osteoarthritis can develop
or progress in patients who have had prior UKA
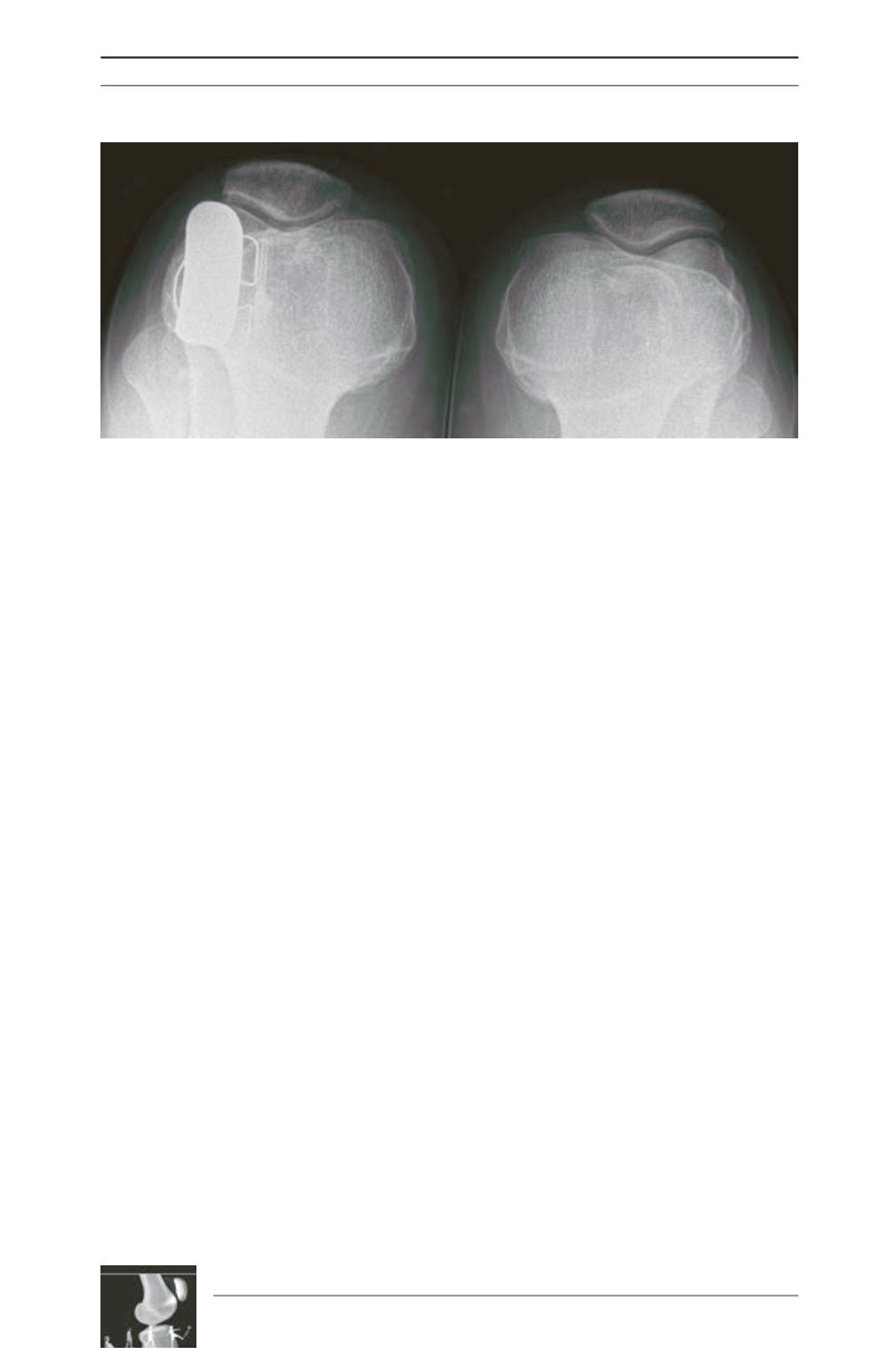
Fig. 2: Patellofemoral articulation without OA (4 years follow-up).