










 302 / 460
302 / 460

Importance and Radiographic Identification of the Femoral Insertion…
301
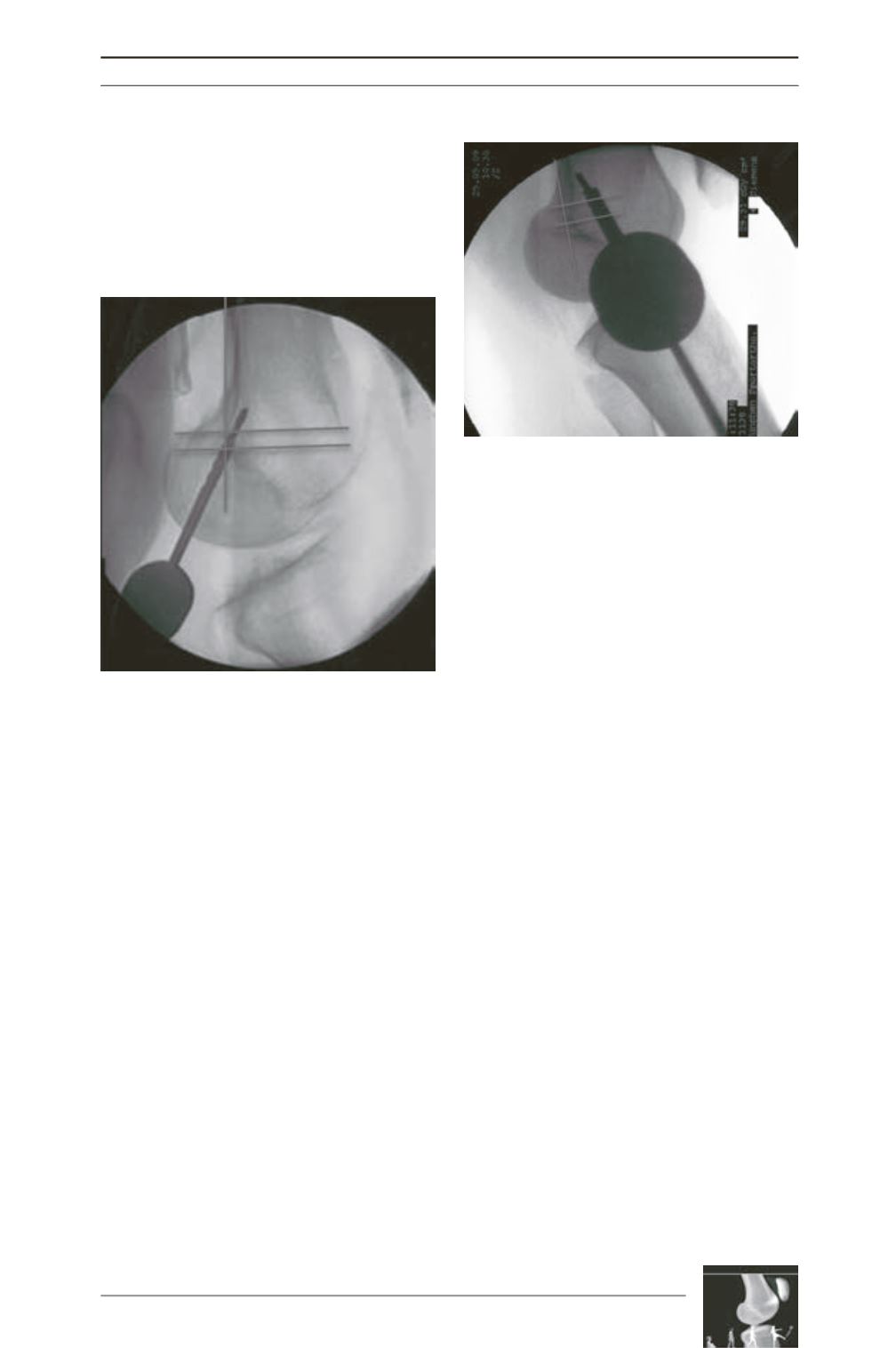
(fig. 3). If this point is deviating obviously or
the cannulated drill is inside the anatomical
insertion area only by 50% (fig. 4), the guide
wire has to be removed and reinserted towards
the desired direction, until an anatomical
positioning is achieved.
Besides the possibility of a very small skin
incision at the femoral side with the maximal
length of the screw diameter, used for the
femoral fixation, the femoral insertion becomes
reproducible and the risk of a non-anatomical
reconstruction can be minimized drastically.
Especially in patients, where the medial aspect
of the distal femur is covered with soft tissue, a
radiological identification of the insertion point
is highly recommended and is simplifying the
operation.
Fig. 3: Intraoperative view by fluoroscope at the
correct position. The insertion point is identified at
the point, where the cannulated drill is attaching
the bone (anterior to the posterior condyle line,
distal to the perpendicular through the inition of
the medial condyle and proximal to the most
posterior point of the Blumensaat line).
Fig. 4: Non anatomical position: the cannulated drill
attaches the bone too far anterior and proximal
Literature
[1] Allen CR, Giffin JR, Harner CD. Revision
anterior cruciate ligament reconstruction.
Orthop Clin North
Am, 34(1): 79-98, 2003.
[2] Amis AA, Firer P, Mountney J, Senavongse
W, Thomas NP. Anatomy and biomechanics of the medial
patellofemoral ligament.
Knee, 10(3): 215-20, 2003.
[3] Bernard M, Hertel P, Hornung H, Cierpinski
T. Femoral insertion of the ACL. Radiographic quadrant
method.
Am J Knee Surg, 10(1): 14-21; discussion 21-2, 1997.
[4] Conlan T, GarthWP J
r
, Lemons JE. Evaluation of
the medial soft-tissue restraints of the extensor mechanism
of the knee.
J Bone Joint Surg Am, 75(5): 682-93, 1993.
[5] Davis DK, Fithian DC. Techniques of medial
retinacular repair and reconstruction.
Clin Orthop Relat Res,
(402): 38-52, 2002.
[6] Desio SM, Burks RT, Bachus KN. Soft tissue
restraints to lateral patellar translation in the human knee.
Am J Sports Med, 26(1): 59-65, 1998.
[7] Elias JJ, Cosgarea AJ. Technical Errors During
Medial Patellofemoral Ligament Reconstruction Could
Overload Medial Patellofemoral Cartilage: A Computational
Analysis.
Am J Sports Med, 2006.
[8] Ellera Gomes JL, Stigler Marczyk LR,
Cesar de Cesar P, Jungblut CF. Medial
patellofemoral ligament reconstruction with semitendinosus
autograft for chronic patellar instability: a follow-up study.
Arthroscopy, 20(2): 147-51, 2004.
[9] Hautamaa PV, Fithian DC, Kaufman KR,
Daniel DM, Pohlmeyer AM. Medial soft tissue
restraints in lateral patellar instability and repair.
Clin
Orthop, (349): 174-82, 1998.