










 357 / 460
357 / 460

V.B. Duthon, P. Neyret, E. Servien
356
completely. A full incapacity to actively extend
the knee is due to a complete rupture of the
quadriceps tendon and of the retinacula. By
palpation of the quadricipital tendon, a gap is
felt, corresponding to an interruption of tendon
continuity. 60% of tears occur through the
tendon, about 2cm above the patella, and 40%
occur at its insertion on the patella. The latter
injury is called “osteotendinous tear” and was
first described by Albert Trillat. It is due to a
periosteal sleeve avulsion at the quadriceps
tendon insertion on the patella. Rarely, the tear
occurs at the myo-tendinous junction, mainly
in patients with a decreased ambulation and
muscular hypotrophy. Swelling and hematoma
due to the rupture can fill this gap and make its
palpation less obvious [7].
The differential diagnosis in a patient unable to
fully actively extend the knee is a paralysis of
the femoral nerve which can be traumatic or
iatrogenic [24].
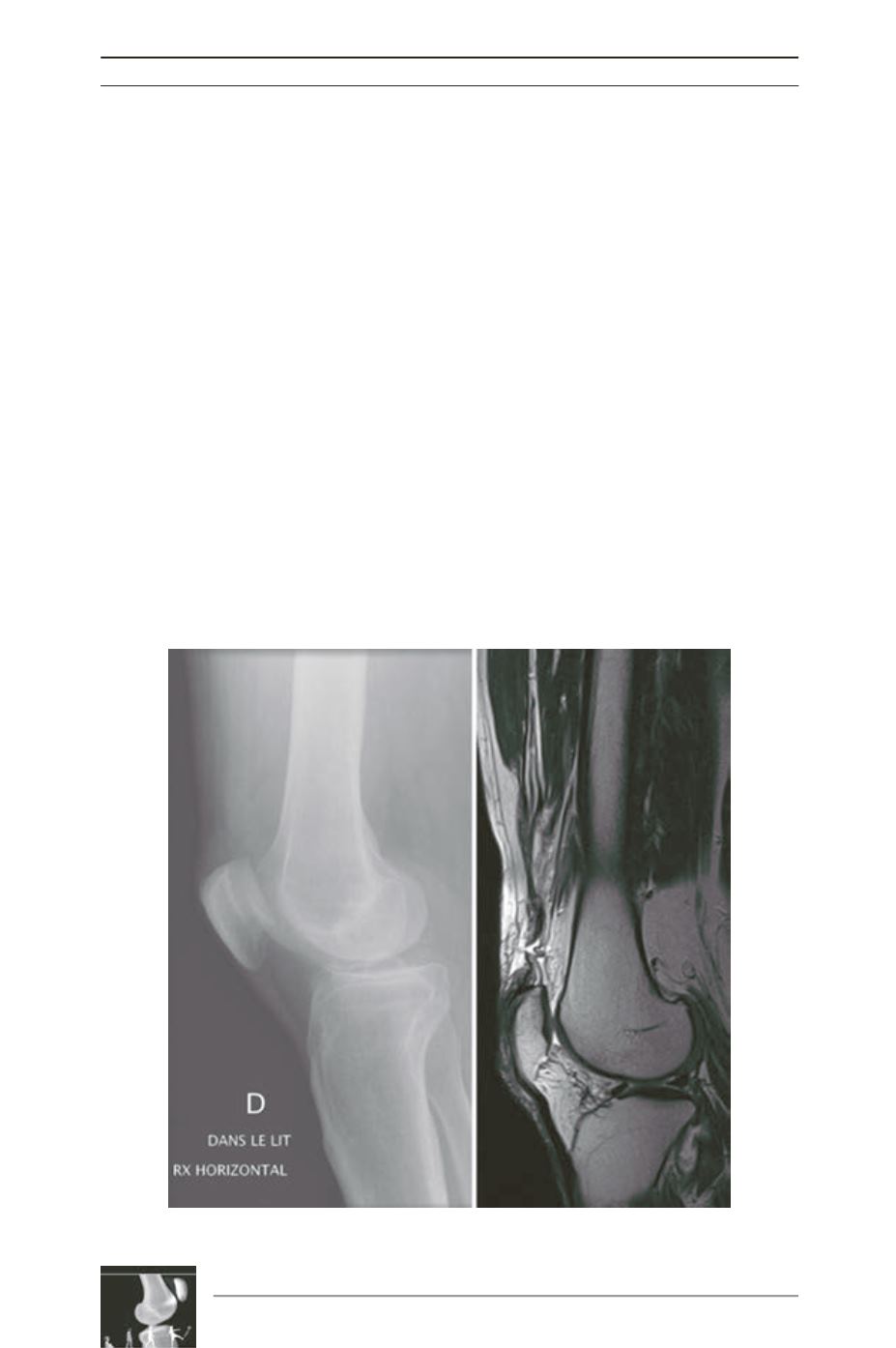
Diagnosis is first made with anamnesis and
clinical exam. Radiological exams can help to
confirm and precise the diagnosis. On a
standard profile radiograph of the knee,
swelling of the soft tissues above the patella
can be seen (fig. 1A). Calcifications on the
proximal border of the patella are an indirect
sign of quadriceps tendinopathy which
predisposes the tendon to rupture [6]. The
patella is lower than on the controlateral side
(patella baja) and may be anteriorely tilted.
Echography is a non-invasive, easy and fast
diagnostic tool to confirm a partial or complete
rupture of the quadriceps tendon. MRI has a
high sensitiviy (fig. 1B) and is recommended
in cases where a doubt persists after clinical
and echographic exam. It also helps to see if
the tear is complete (the 4 layers of the tendon
are torn) or partial, and if the retinacula are
torn [7].
Fig. 1
A
B