








 112 / 242
112 / 242

V. Villa, A. Madelaine, T. Lording, S. Lustig, E. Servien, P. Neyret
112
blade osteotome was introduced into the
epiphysis for optimal fixation, with an entry
point proximal and anterior to the origin of the
lateral collateral ligament.
The optimal obliquity of the blade in relation to
the joint line depends on the location of the
deformity and the magnitude of the desired
correction.
The osteotomy was performed using a saw, at
least 25mm from the entry point for the blade
plate to ensure an adequate cortical bridge. The
blade plate was then introduced. The medial
cortex was weakened by perforation with a
guide wire, taking care to maintain cortical
continuity.
The osteotomy was opened using two or more
Lambotte osteotomes, whilst the blade plate
was impacted. The opening and impaction was
continued until the plate was in contact with
the lateral cortex of the femur. Fixation was
then completed in the diaphysis using bicortical
4.5mm screws above the level of the osteotomy.
The osteotomy was grafted using cortico-
cancellous autograft from the ipsilateral iliac
crest.
Operative data were collected, and pre- and
post-operative alignment and leg length were
measured.
Results
The mean osteotomy opening was 8.3° (5°-
13°). The femoro-tibial mechanical axis
(mFTA) was improved significantly, from
187.8° (183.0°-197.0°) to 180.4° (176.0°-
186.0°) post-operatively (p<0.001), without
loss of correction over the follow-up period
(fig. 1 et 2). The pre-operative leg length
discrepancy was -0.7cm, compared to -0.6cm
post-operatively, which was not significant.
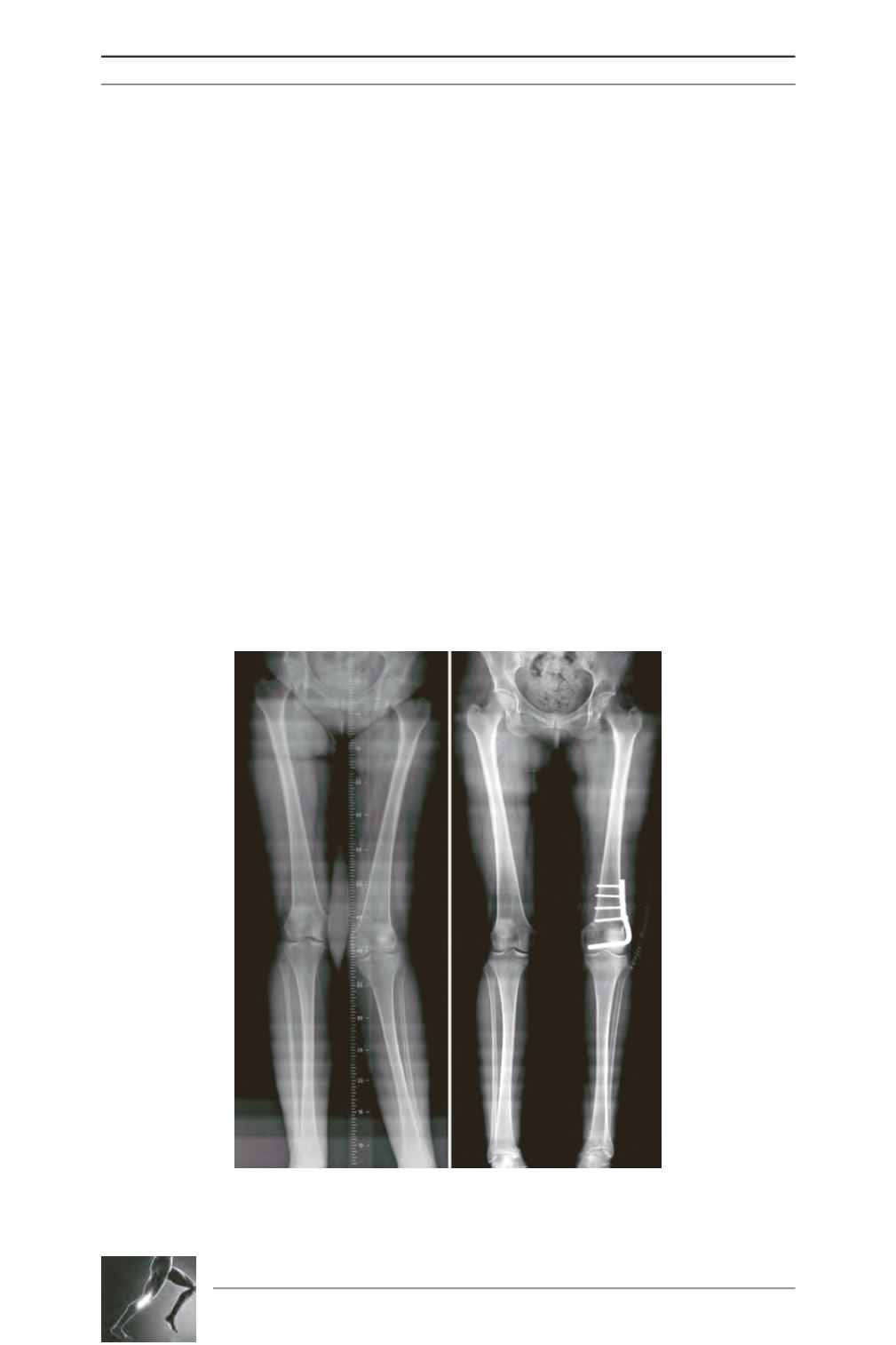
Fig. 1: Pre and postoperative long leg views of a 40 year old patient
with idiopathic genu valgum. mFTA improved from 197° to 178° on
the immediate postoperative long leg view.