








 197 / 242
197 / 242

What are the limits for Unicompartimental Knee Arthroplasty?
197
Correction of flexion
deformity
Many surgeons consider flexum deformity as
an absolute contraindication for UKR. Before
evaluate flexum as irreducible and consider
TKR as the unique solution, some tips should
be performed.
First of all, evaluate it under anesthesia. Often
flexum is only a consequence of knee pain.
After that, give space to the ACL! Removing
any osteophyte from the notch will free the
ACL. Then, remove any posterior osteophyte.
This should be done after tibial and femoral cut
to obtain enough space for working posteriorly.
After component trial position, range of motion
should be tested. If some degrees of flexum are
still present, a dosed elongation of the knee
flexors should be done. To do this, no surgical
acts should be done. Agentle manual stretching
is enough. This procedure takes time because
theknee shouldbemaintained inhyperextension
for some minutes, but it is very effective.
Undercorrection of
the deformity
Tibio-femoral wear in knee osteoarthritis (OA)
often causes varus or valgus deformity. The
location of tibio-femoral wear (medial or lateral
compartment) is often a consequence of the
morphotype [12].
A native valgus knee can develop lateral OA,
a native varus knee can develop medial OA.
Osteoarthritis worsens the amount of the
deformity, and this fact should be considered
in UKR. The tibial and femoral cuts should
be done in order to correct the deformity
caused by cartilage wear, not the one
determined by the morphotype. The aim is to
respect the joint line. Postoperative
mechanical axis should be hypo-corrected,
proportionally to preoperative deformity and
constitutional varus-valgus (fig. 3). This
shrewdness will not alter the native knee
biomechanic and will not cause overstress on
the opposite compartment.
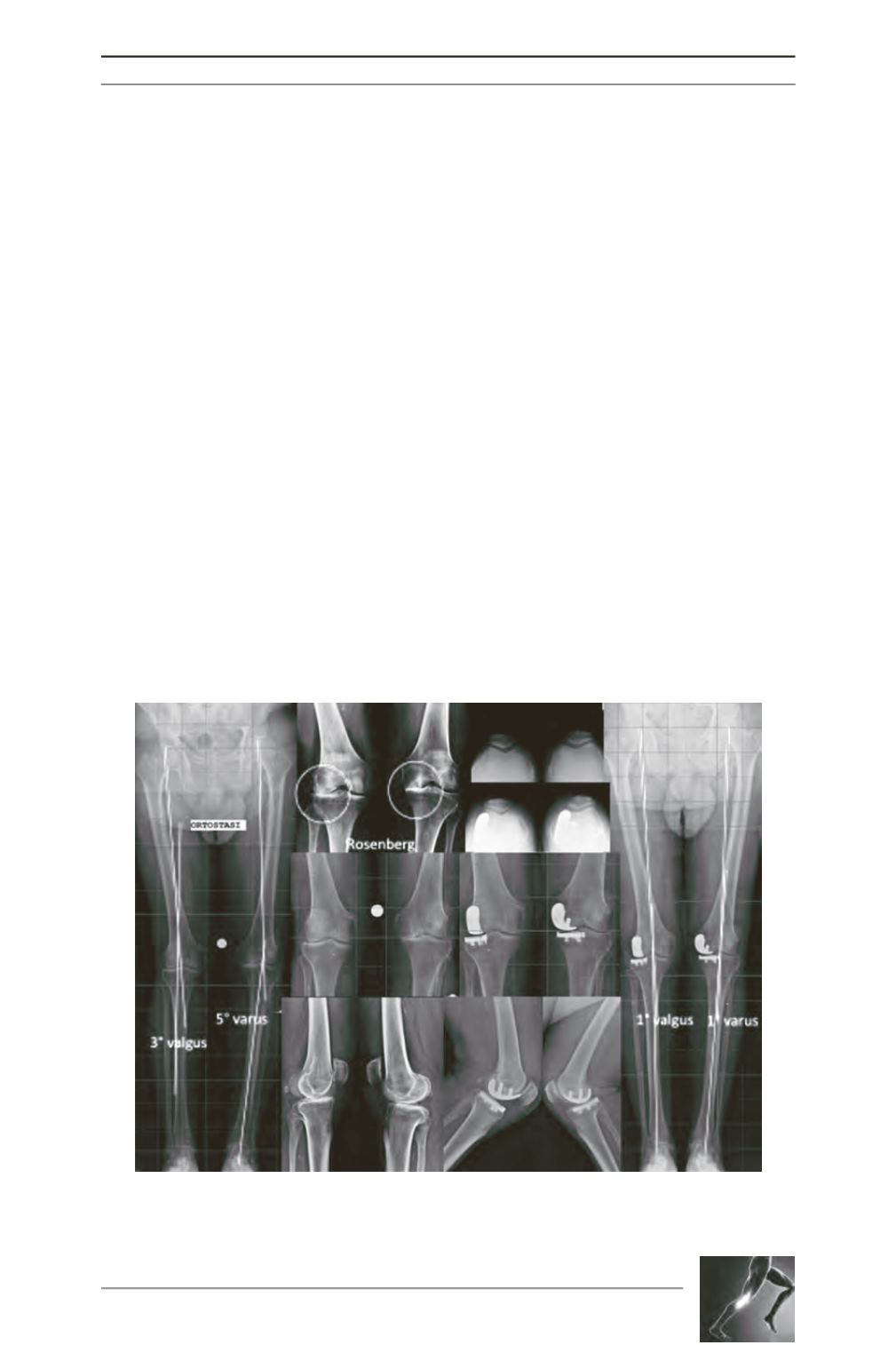
Fig. 3: 83 years old man with right knee lateral OA and left knee medial OA. He had simultaneous
bilateral UKR. Postoperative X-rays showed undercorrection of the coronal deformity to respect
the native morphotype.