










 229 / 324
229 / 324

cement is antibiotic loaded Palacos (62.1% of
cases) [14]. The current cost of these compo-
nents prior to any locally negotiated discounts
was obtained from the implant company repre-
sentatives. The sum cost for each procedure
was calculated based on these figures and
quantitatively compared based on current NJR
usage figures. Those elements of the surgical
procedure that are not known differ consistent-
ly between UKA and TKA were excluded
from calculations. Equivalent costs were assu-
med for theatre and medical staff, theatre
consumables, instrument sterilisation, dres-
sings, IV fluids, and peri-operative drugs and
anaesthetic agents.
The hospital episode
The NJR has published data on the average
length of stay (LOS) for TKA and UKA based
on 73,967 cemented TKA and 4,484 UKA pro-
cedures carried out between April 2003 and
September 2006 [14]. The cost of a day in an
NHS hospital orthopaedic ward was estimated
using figures provided by the management
team in our institution (Charing Cross
Hospital, London) for the running of our
20 bedded ring fenced elective orthopaedic
ward. These data were combined with current
LOS figures from the NJR to estimate the cost
of the hospital episode for each TKA and UKA
procedure. Elements of the hospital stay that
do not differ consistently between UKA and
TKA were excluded from analysis. These
included the cost of pre-operative or post-ope-
rative investigations, IV fluids, compressive
stockings and dressings.
The cost of an active contraint robotic
UKA
The cost of custom made prostheses using
modern manufacturing processes was establi-
shed, and the cost of manufacture of a current
active constraint robot with a maintenance
contract and disposables calculated based
upon a usage of 50 and 100 cases a year.
RESULTS
Applicability of UKA
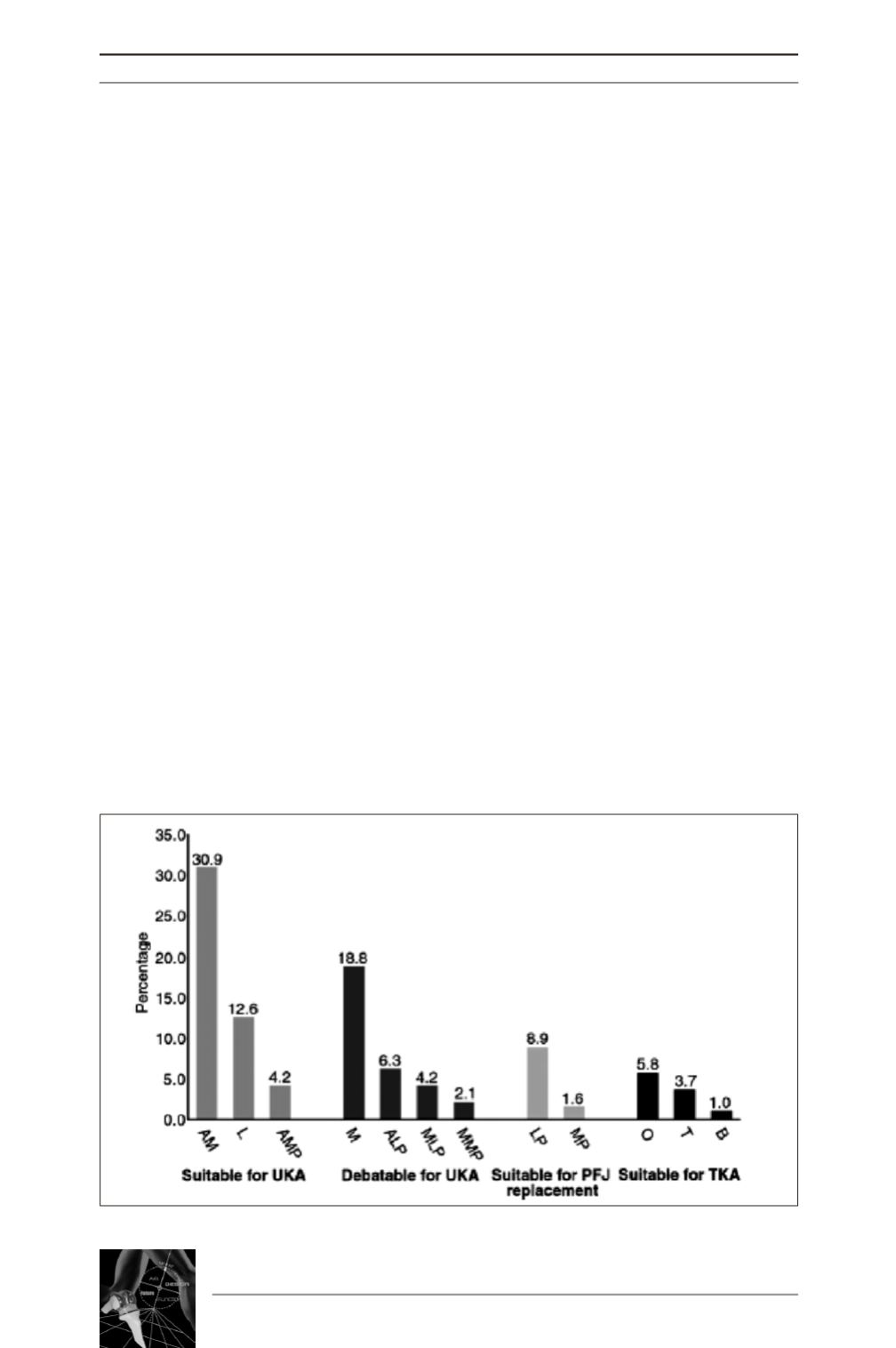
Of the 200 knees reviewed, 9 cases undergoing
surgery for revision or rheumatoid arthritis
were excluded. The remaining 191 radio-
graphs were categorised as shown in Figure 1.
14
es
JOURNÉES LYONNAISES DE CHIRURGIE DU GENOU
228
Fig. 1 : Histogram showing the distributing of patterns of knee arthritis