








 165 / 242
165 / 242

165
Every surgeon aims to safeguard their patient’s
future. This can be accomplished through two
different strategies: keep doing what one has
always been doing because it works well, or
take some risks to try to make things better.
The purpose of this analysis is not to provide
an unambiguous course of action; instead we
wanted to define the role of cementless total
knee arthroplasty (TKA) based on a review of
literature. We also wanted to define a set of
specifications for cementless TKA.
We are not trying to put cemented TKA – the
current gold standard – on trial. It is safe, can
make up for imperfections in the bone cuts and
has a low rate of loosening over time. In revision
cases, there are fewsurprises except for cemented
long stems. But cemented implants have their
drawbacks: the rare case of cement-related
shock, release of foreign bodies or particles that
can cause premature implant wear. The ageing
of the cement over the long-term also has some
unknowns. And since it takes up and alters the
space made by the bone cuts, it can lead to
stiffness and pain or alter the alignment. Few of
us check the alignment when we apply the
cement, even though navigation systems with
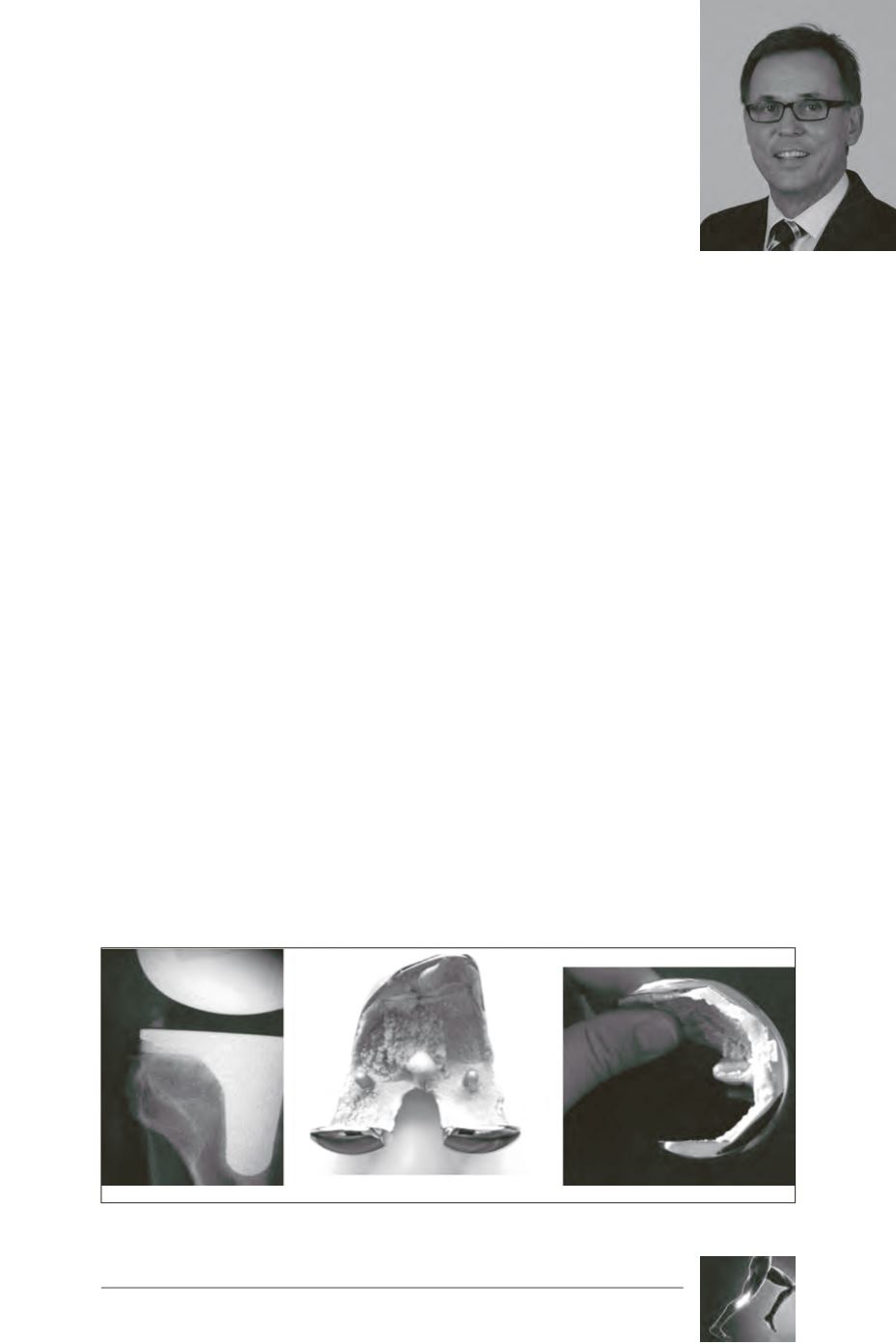
0.5° precision are available. Cement (fig. 1) can
also cause up to a 2° change in the alignment.
What is the future of cemented implants? An
overly easy explantation (fig. 2) reminds us of
the possibility of problems at the bone-cement
interface.
Strategy: which implant for
which patient?
Specific considerations
about TKA in young patients
Protecting the future: Cemented or cementless
O. Courage, V. Guinet, L. Malekpour
Fig. 1
Fig. 2