








 160 / 242
160 / 242

R. Bastos-Filho, P. Neyret
160
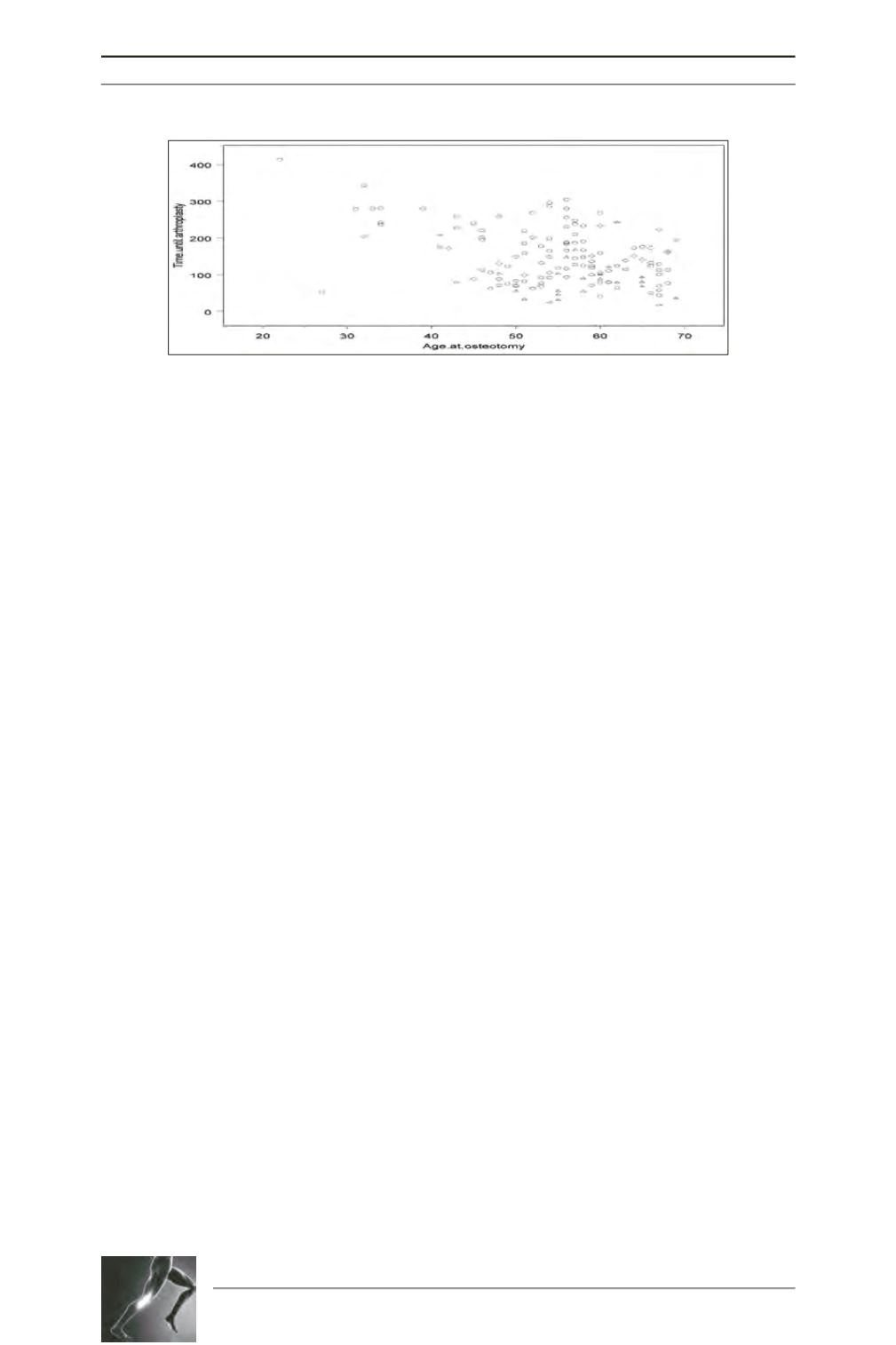
We also identified a significant linear
relationship (p = 0.0025) between patient age
at the time of osteotomy and the time until
arthroplasty. Younger patients exhibited longer
osteotomy survival until arthroplasty than did
older patients (r = -0.2588318) (fig. 3).
Discussion
The most important result of this study is that
the osteotomy surgical technique (OWO or
CWO) influences the survival rate of this
surgery. To our knowledge, no previous study
has compared survivorship between CWO and
OWO. We consider this point to be extremely
important because the goal of HTO for the
treatment of osteoarthritis is to delay the
performance of TKA. Thus, a higher survival
rate indicates a more effective procedure.
Another factor to note is that CWO can be fixed
with minimal osteosynthesis hardwire and with
satisfactory stability because of good bone
contact; thus, the final cost is lower. The reason
for the frequency of reversal in the surgical
indications for CWO to OWO in the literature
is unclear. The latter technique is currently
much more common despite its higher cost.
While lateral CWO theoretically distalizes the
joint line and increases patellar height [12, 13],
clinical evidence indicates that patella infera is
actuallymore common following this procedure
[15-17]. This finding may be a consequence of
postoperative immobilization and subsequent
scarring of the patellar tendon in this population.
Opening-wedge HTO also predisposes to
patella infera, as demonstrated in several
clinical studies [11, 13, 17]. These prior
findings were confirmed in our study. Both
groups demonstrated a lower overall pre-TKA
patellar height.
Insall revised the HTO results between 1960
and 1990 and concluded that younger patients
with moderate varus deformity had better
results [18]. Our study findings are consistent
with this information. We found a linear
(p=0.0025) relationship between patient age at
the time of the osteotomy and the delay until
performance of TKA. Thus, the younger the
patient, the greater the osteotomy survival time
until arthroplasty (r = -0.2588318). This finding
can be explained by the higher bone quality
and existing cartilage in younger patients.
A recent study comparing these two osteotomy
techniques concluded that the radiographic
alignment, functional outcomes, goals, and
complication rates were equal in patients who
underwent TKA by CWO and OWO.19
However, the survival rates of the osteotomies
were not addressed in that study.
This study had several limitations. First, in our
comparison of OWO and CWO, we did not
compare randomized groups of patients, but
rather patients that underwent one procedure or
the other for a variety of undefined reasons.
Table 1 demonstrates that the groups were
Fig. 3: Osteotomy survivorship according to age. Circles represent
closing-wedge osteotomies, and triangles represent opening-wedge osteotomies.