








 222 / 242
222 / 242

A. W-Dahl, L. Lidgren, M. Sundberg, O. Robertsson
222
In 2013, UKA constituted 4% of the knee
arthroplasty surgery and was most commonly
used in the age group of 55-64 years. About
18% of the UKA surgery was performed in
patients younger than 55 years of age. 39 out of
73 hospitals performed UKA in 2013 compared
to 60 out of 76 in 2007.
While TKAand UKAare used in all age groups,
HTO is mostly considered in the younger and/
or physically active patients. The SKAR has
provided information on the knee arthroplasty
surgery since 1975 while the information on
HTO has been lacking.
In the beginning of the 1980s, HTO was
estimated beeing 30% of the primary knee
reconstruction surgery in Sweden (Tjörnstrand
et al.
1981), decreasing to about 20% during
the period 1989-1991 (Knutson
et al.
1994). In
a population based study using information
from the Swedish National Board and Health’s
register for 1998-2007, verifying laterality and
diagnosis by medical records, it was shown
that the use of HTO has decreased by 30%
during these years amounting for 6.8% of the
primary knee reconstruction surgery in 1998,
as compared to 2.5% in 2007 (W-Dahl
et al.
2012). Similar information from the Swedish
National Board of Health and Welfare,
estimated HTO’s to be less than 2% of the knee
reconstruction surgery for knee OA in 2012.
The SKAR has shown that the revision rates in
younger patients operated on by TKAand UKA
increase by younger age and that the risk of
revision at 10 years for TKA and UKA are
doubled for patients younger than 55 years of
age as compared to those 55 years and older
(fig. 2) with no differences between men and
woman (W-Dahl
et al.
2010). The risk of
revision for HTO increased by older age and
was higher in woman than men. The risk of
being converted to a knee arthroplasty at
10 years was 30% (fig. 3).
Most of the osteotomies performed during
1998-2007 were done in clinics performing
less than 15 operations a year. For UKA, it has
been shown that hospitals performing less than
23 UKAs a year had a 1.6 times higher revision
rate than units that performed more (Robertsson
et al.
2003). It is not unlikely that similar
factors influence outcome in HTO. The use of
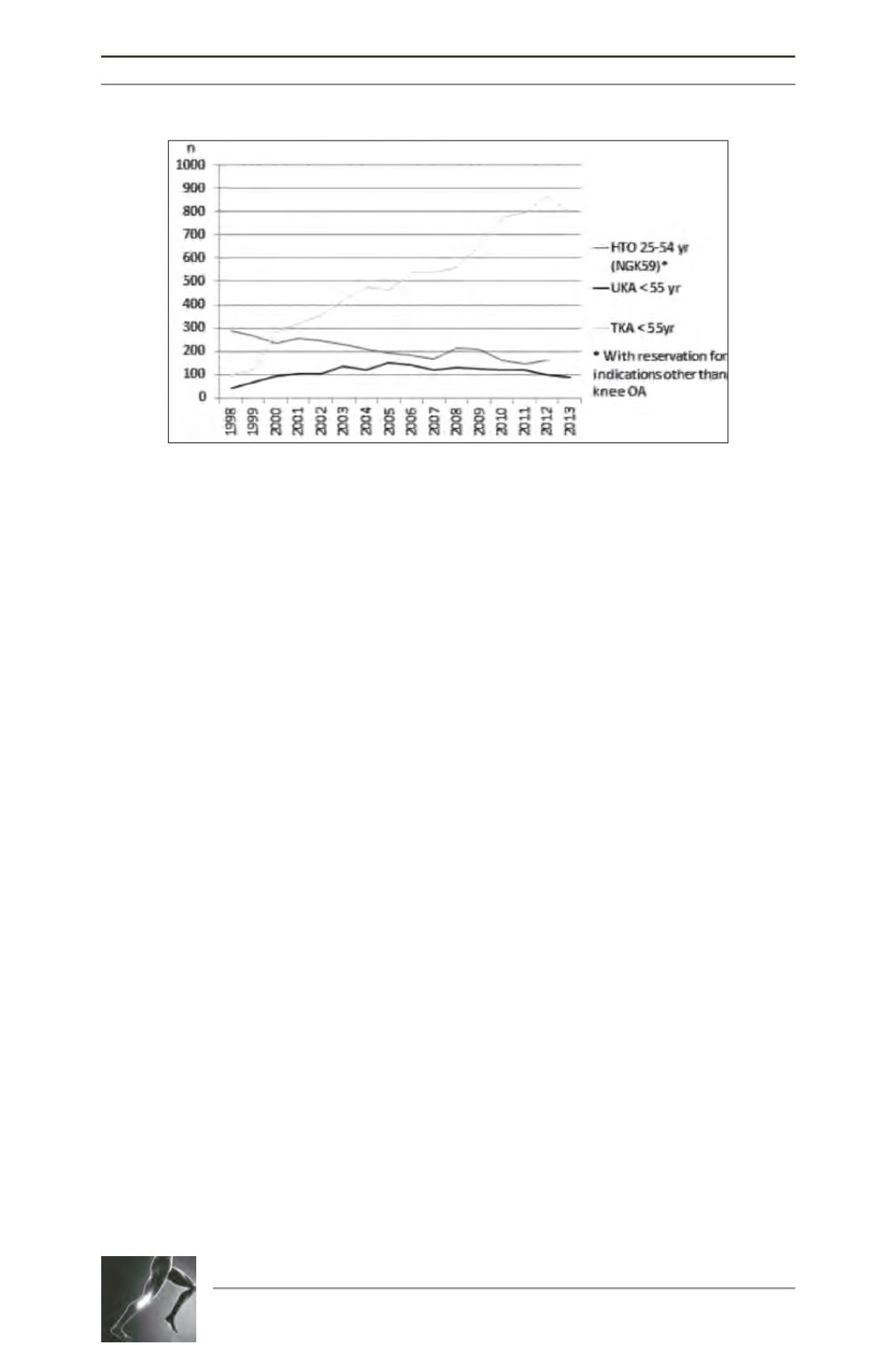
Fig. 1: High tibial osteotomy* (HTO), uni-compartmental knee arthroplasty (UKA) and
total knee arthroplasty (TKA) for knee osteoarthritis in patients younger <55 years of
age 1998-2013. Sources: The Swedish Knee Arthroplasty Register and the Swedish
National Board of Health and Welfare.