








 67 / 242
67 / 242

Anatomy, kinematics an knee prostheses; 3D variations in knee anatomy?
67
Indeed, although many authors have studied
normal lower leg alignment in humans before,
this finding has been unrecognized so far. Some
of the reasons for this are the fact that many
classic alignment studies have been flawed
with a number of shortcomings, such as a
limited number of participants, a large
variability in the subjects’ age, recruitment in a
hospital setting, lack of stratification, and
selection bias of the subjects.
The association of constitutional varus
alignment with increased physical activity
during growth has been raised by other authors
before. Witvrouw
et al.
have noted that intense
sports activity during growth leads to the
development of varus knees, and this
phenomenon occurs especially towards the end
of the growth spurt [30].
We believe that such is the consequence of
Hueter-Volkmann’s law, which states that
growth at the physes is retarded by increased
compression, whereas reduced loading
accelerates growth [25, 28, 29]. The increased
loads caused by the adduction moment on the
knee during ambulation and physical activity
leads to the development of varus alignment
secondary to delayed growth on the medial
side and accelerated growth on the lateral
physes. Cooke and Lavernia have in the past
already alluded to this theory in a
biomechanical study on the etiology of
pediatric tibia vara [12].
The observations from our study have proven
that an important variability in natural
alignment exists amongst individuals. One
should therefore question the dogma that zero
degree mechanical alignment should be the
goal in every patient undergoing TKA.
Restoring the alignment to neutral in patients
with constitutional varus would indeed be
abnormal and in fact unnatural for them, since
it would implicate an overcorrection towards
their natural situation in which they had spent
their life since skeletal maturity.
A strategy where the natural alignment of the
patient is determined and subsequently repro
duced, seems therefore much more logical.
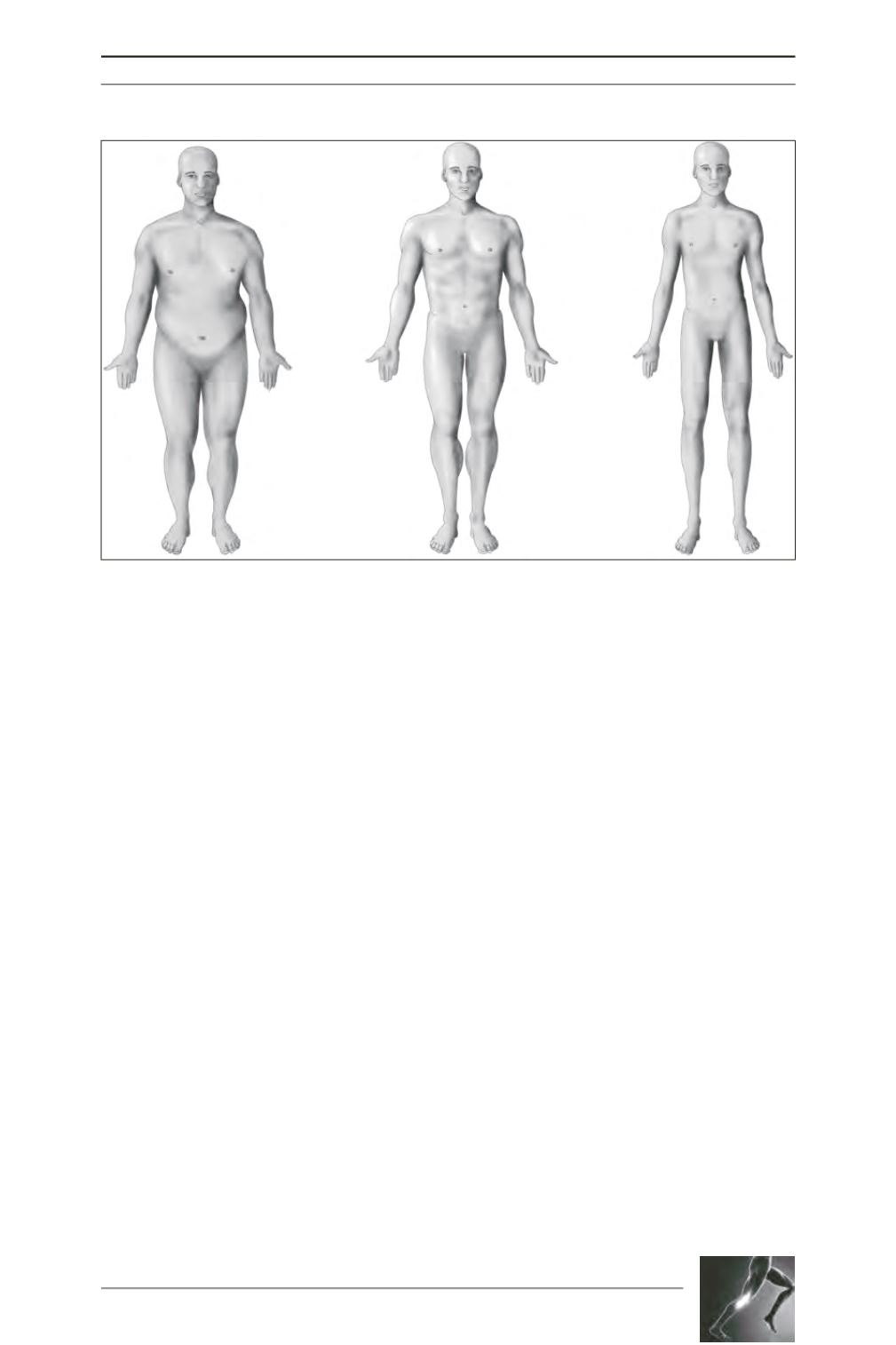
Fig. 2: Together with gender, the patient’s morphotype is another important predictor of the shape of the
knee. The three basic morphotypes are endomorph (left), mesomorph (middle), and ectomorph (right) [3].