










 104 / 244
104 / 244

WHY DO I PREFER OUTSIDE-IN IN ANTERIOR CRUCIATE LIGAMENT RECONSTRUCTION?
103
Then, the tibial guide is positioned through the
AM portal, using as anatomic landmarks the
posterior border of the anterior horn of the
lateral meniscus, the anterior border of the
PCL and the interspinous area. The tibial guide
has to be set with an orientation between 55°
and 65° regarding the horizontal plane and
with a 25° of inclination in the sagittal plane of
the tibia, close to the medial collateral
ligament. Finally the tibial pin is drilled and its
position is tested during the range of motion to
ensure that there is no impingement. The tibial
and femoral tunnels are performed using a
6mm drill. The pins are adjusted according to
ACL fibers orientation and the tunnels are re-
drilled according to proper graft size (fig. 4).
Tunnel lengths are measured. The graft is
passed in the tunnels through pulling sutures.
BPTB graft is pulled from the femoral to the
tibial tunnel. The trapezoidal tibial bone block
should be inserted in the femoral tunnel with
the cancellous bone facing forward. The
patellar block is pulled into the tibia, and 90°
internally rotated in order to simulate the ACL
bundles orientation. Then, femoral press-fit
fixation is achieved. It is recommended to tap
the tibial block until it is flush with the tunnel
entry point at the articular side. When
hamstring tendons are detached, the graft
passage is performed similarly from the
femoral to the tibial tunnel. In case of the tibial
insertion is preserved, the graft is pulled from
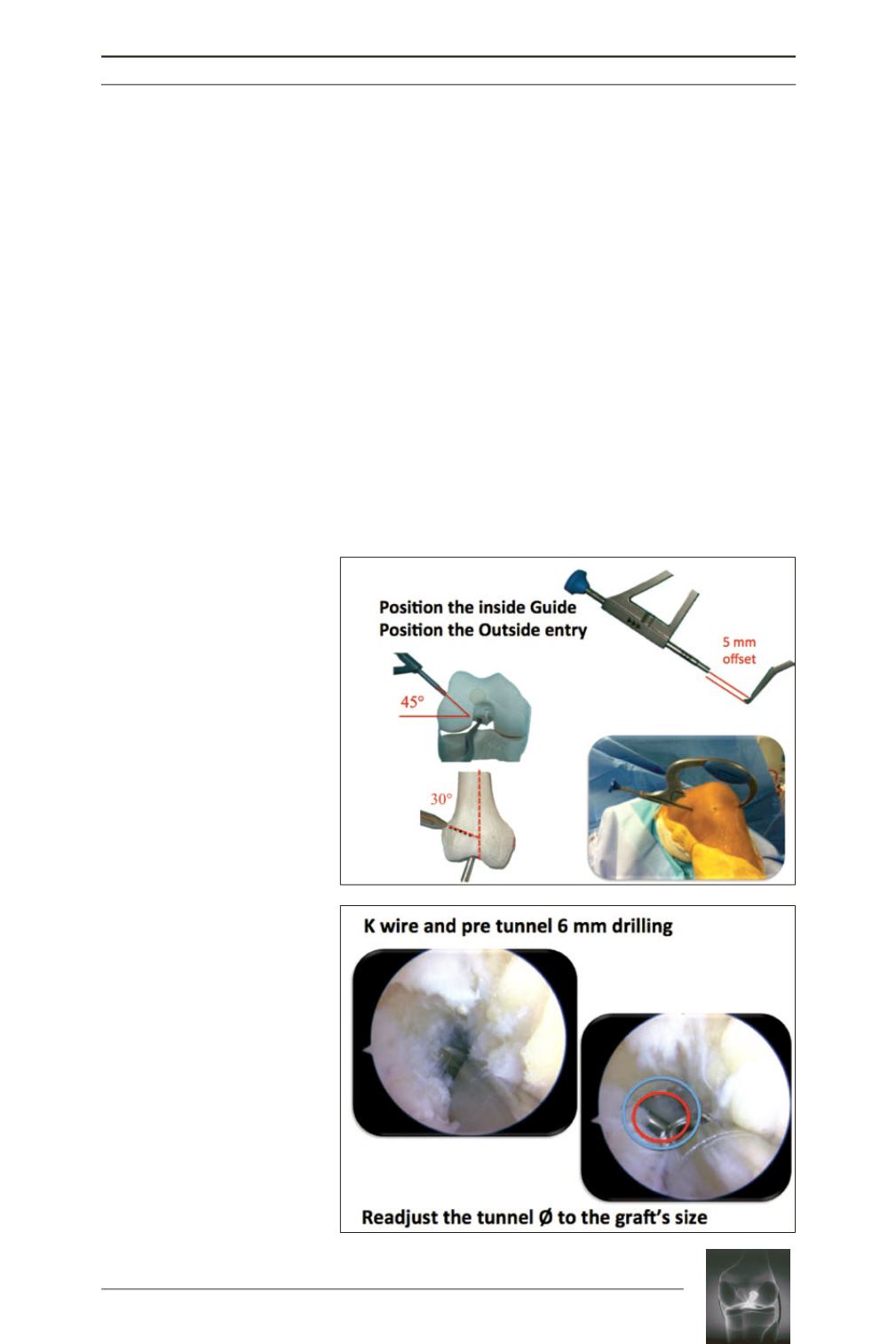
Fig. 3:
5 mm offset outside-in
femoral guide is positioned at
ACL femoral insertion site with an
orientation of 45° in the axial
plane and 30° in the frontal plane.
Fig. 4:
After K wire positioning;
the femoral pre tunnel is
performed with 6mm drill. The
pins are adjusted according to
ACL orientation and the tunnels
are re-drilled according to the
proper graft size.