










 152 / 244
152 / 244

ANTERIOR CRUCIATE LIGAMENT AUGMENTATION
151
remnant. Whilst it is true that the femoral
attachment of the ACL is mainly on the
resident’s ridge, the grafted tendon is pulled
and shifts to the anterodistal side of the femoral
tunnel opening in the knee extension and mild
flexion position. Therefore, our thinking at this
point is that the center of the femoral tunnel
opening should not be on the resident’s ridge,
but should be placed just behind the resident’s
ridge when using hamstring tendon for ACL
reconstruction [1].
Partial rupture of the ACL is an ideal indication
for ACL augmentation. In cases of partial
rupture, single-bundle reconstruction of the
ruptured bundle is desirable, to minimize
damage to the ACL remnant. However, it may
be true that the remaining AM or PL bundle is
not completely intact and that the biomechanical
function of the remaining bundle declines to
some extent. Therefore, in cases of PL bundle
rupture, the central portion of the femoral
tunnel should not be the center of the femoral
attachment of the PL bundle. It is recommended
that approximately three-quarters of the
femoral tunnel opening is occupied by the
femoral attachment of the PL bundle and
approximately one-quarter by the femoral
attachment of the AM bundle. The same goes
for AM bundle rupture. As for the patients with
a thickACL remnant between the intercondylar
notch and the tibia after complete ACL rupture,
the positions of the femoral tunnels is the same
as used for standard anatomic single-bundle
ACL reconstruction.
Tibial bone tunnel
A longitudinal slit is made at the center of the
ACL remnant through the anteromedial portal.
The ACL tibial guide, with the angle set at 60°,
is used to pass a guide pin or Kirschner wire.
The tip of the tibial drill guide is placed through
the slit of the ACL remnant. In cases of PL
bundle rupture, the tibial tunnel is positioned
in the center of the tibial insertion of the
whole ACL. In cases of AM bundle rupture
and complete rupture, the tibial tunnel is
located just posteriorly to the anterior margin
of the footprint.
Graft passage and fixation
The graft composite is introduced from the
tibial tunnel to the femoral tunnel. In cases of
PL bundle rupture, if the graft passes above the
ACL remnant, the positional relationship is
anatomically incorrect. Therefore, in cases of
PL bundle rupture (fig. 1) and complete rupture,
the graft passes through the slit of the ACL
remnant. However, in cases of AM bundle
rupture, the graft passes above the ACL
remnant (fig. 2). After passage of the graft
composite, the proximal side of the graft is
fixed to the lateral femoral cortex by flipping
the Endobutton. Then, a tension force of 50 N
is applied to the distal Endobutton tape
connected to the graft, and the grafted tendon is
fixed at 30° of knee flexion using two staples
(double stapling technique). We also perform
double-bundle reconstruction with the
remnant-preserving technique (fig. 3).
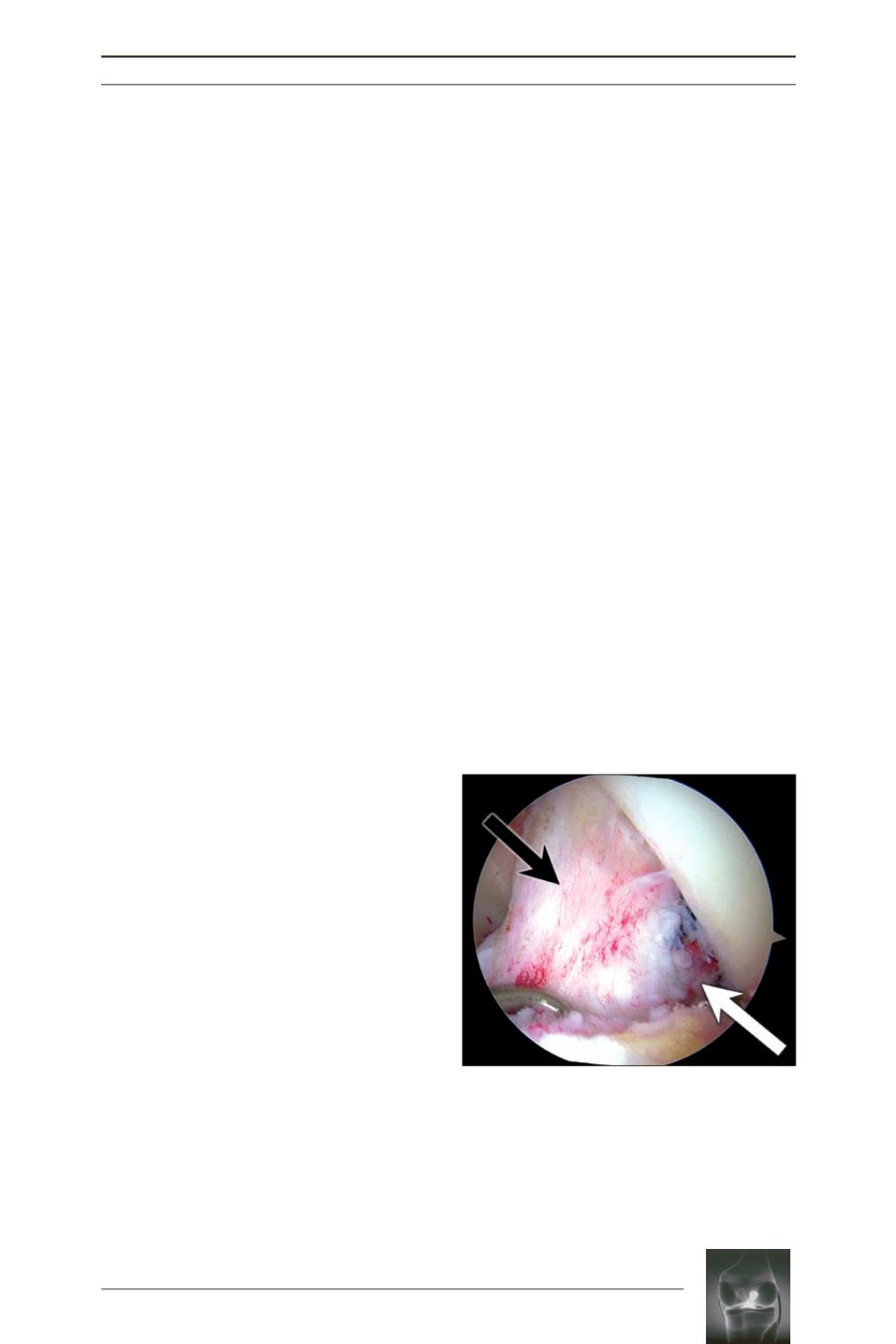
Fig. 1:
Anteromedial (
AM
) bundle- preserving ACL
augmentation for posterolateral (
PL
) bundle
rupture (white arrow, grafted tendon; black arrow,
preserved AM bundle).