










 157 / 244
157 / 244

G. ESTOUR, A. PINAROLI, L. BUISSON
156
From this anatomic risk factor, several studies
have described a revision of an ACL re
construction, a tibial deflexion osteotomy to
correct the tibial slope. It’s suggested that
correction is needed when the angle is over 12°
and it can reduce the risk of recurrent failure.
The technique is an anterior closing wedge
tibial osteotomy with or without detachment of
the patellar tendon [6].
Intercondylar notch stenosis
The shape of the femoral notch at the anterior
outlet has also been associated with ACL
injury.
This intercondylar notch has been described by
radiographics, MRI, arthroscopy and cadaveric
studies. The U shape is not always identified by
the same anatomic description. Stenosis is
made by a bony ridge on the anteromedial
notch or a narrow apex.
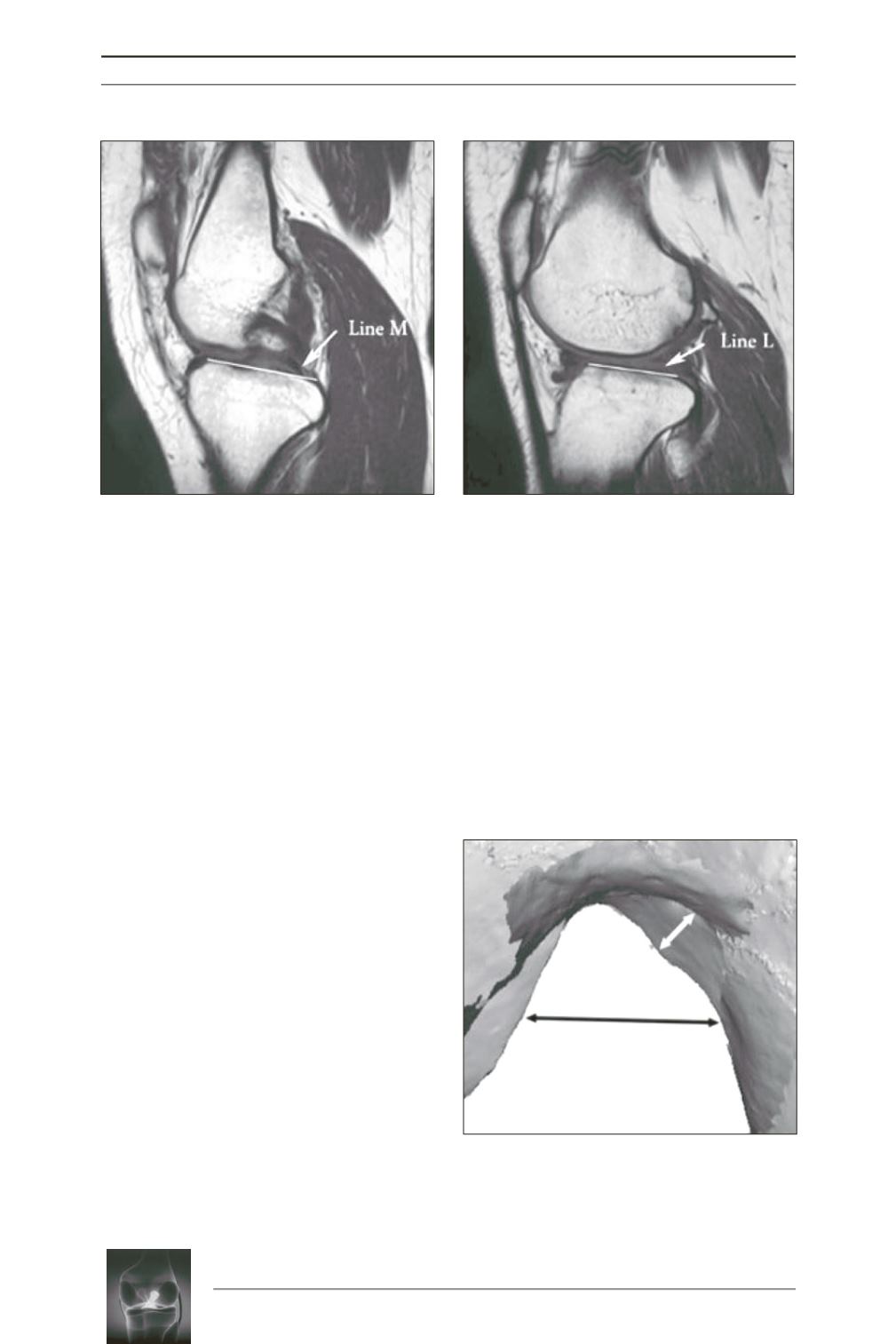
Notch width (black arrows) is measured
halfway between the notch roof and floor; ridge
thickness (white arrows) is measured
perpendicular to the adjacent notch wall at its
widest portion From Joshua S. Everhart [7].
But literature is controversial. One point is the
technique and the mesure of the intercondylar
notch. The second point is the mechanism of
failure. Most ACL injuries are known to occur
with the knee in partial flexion. Most failures
occur close to the femoral attachement site. An
impingement mechanism would brake the
ACL’s need near the stenosis [7].
From Haschimi et al.
[5]
Reconstruction of the notch