










 56 / 244
56 / 244

THE ILIOTIBIAL BAND WITH ITS FEMORAL ATTACHMENTS AT THE KNEE…
55
BIOMECHANICAL STUDIES
OF LATERAL SOFT TISSUES
In our lab at Imperial College, London, a
classic cutting study using a 6-degree-of-
freedom robot was undertaken [9]. Sequentially
structures were sectioned and the same motion
was replayed by the robot, whilst measuring
the resistance to movement. In this way the
percentage contribution to resisting certain
movements could be calculated for the
structures that had been cut. This was
undertaken with the knee at straight, 30, 60 and
90 degrees. As one would expect, throughout
the range of motion tested the anterior cruciate
ligament is the primary restraint to anterior
tibial translation.
Fig. 2:
Lateral soft tissues exposed by refection
of ITB.
Lateral aspect of a left knee: the femur extends
proximally to the right, and the tibia extends
distally toward the bottom left with the patella at
the top left:
1
), Superficial layer of the iliotibial tract
(ITT) flapped down;
2
) proximal femoral insertion of
the ITT;
3
) supracondylar insertion of the ITT;
4
) retrograde insertion or capsulo-osseous layer;
5
) superior genicular artery;
6
) lateral collateral
ligament;
7
) fibular head;
8
) Gerdy tubercle; and
9
) intermuscular septum.
(Courtesy of Am J of
Sports Med)
.
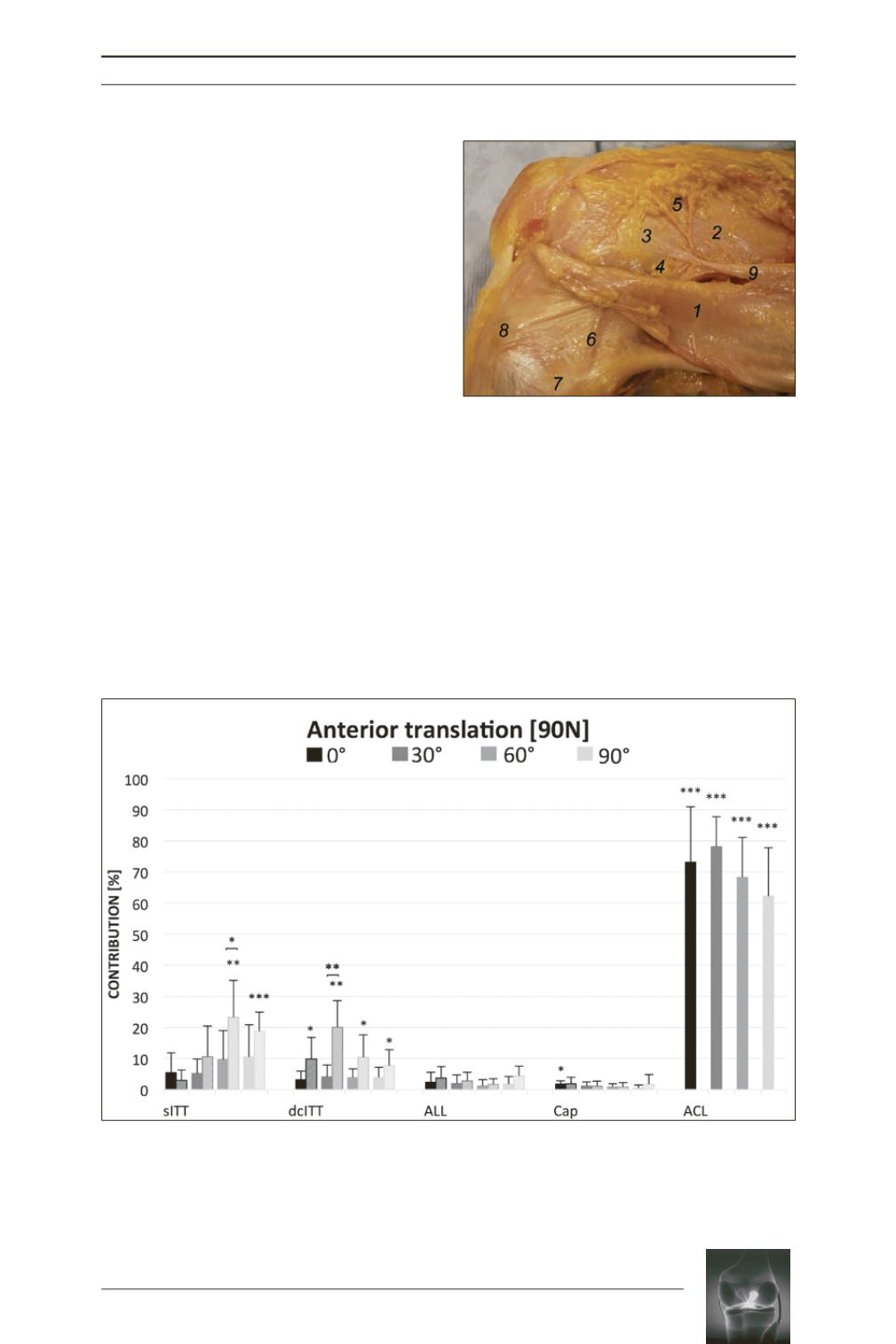
Fig. 3:
Contribution of tested structures in restraining 90-N anterior tibial translation at 0°, 30°, 60°, and 90°
of flexion. Crosshatched areas indicate results from the ACL-deficient group. Shown as mean + SD; n=8.
Statistically significant change from the initial knee state (brackets indicate significant difference between
ACL intact
vs
deficient): *
P
<.05, **
P
<.01, and ***
P
<.001.
ACL
, anterior cruciate ligament;
ALL
, anterolateral
ligament;
Cap
, anterolateral capsule;
dcITT
, deep and capsulo-osseous layer of the iliotibial tract;
sITT
,
superficial layer of the iliotibial tract.
(Courtesy of Am J of Sports Med)
.