










 55 / 244
55 / 244

A. WILLIAMS
54
THE ANTEROLATERAL
LIGAMENT
In recent times the first description of an
“anterolateral ligament” was in a study from
Lyon [2]. Shortly before this the senior author of
the aforementioned article, P
r
Philippe Neyret,
collaborated with a group at Imperial College,
London, to set out the logic for lateral soft tissue
surgery with ACL reconstruction [3] but it was
following an article in 2013 by Claes
et al.
[4]
that an extraordinary amount of interest was
shown, even in the popular press and social
media. In this study embalmed Cadavers were
dissected to demonstrate a structure on the
lateral side of the knee termed the “anterolateral
ligament”. The authors described a well-defined
attachment to the tibia midway between the
lateral collateral ligament (LCL) attachment to
the fibular head and Gerdy’s tubercle. But their
description of the attachment of the femoral end
of the ligament was vague. A few months later
another article from Imperial College by Dodds
et al.
[5], which employed dissection of fresh
frozen Cadavers confirmed the tibial attachment
described by Claes
et al.
[4] and defined the
correct position of the femoral attachment
proximal and posterior to the LCL attachment to
the femur.
Subsequently published collaboration between
Steven Claes and Robert LaPrade’s group [6]
confirmed the femoral attachment described by
Dodds
et al.
[5].
As is often thewaywith anatomic “discoveries”,
the anterolateral ligament has almost certainly
been described previously in many publications
but with different naming. For example as long
ago as 1976 Hughston
et al.
[7] described the
“mid third capsular ligament”.
Many studies have been published recently that
seem to confirm the existence of an anterolateral
ligament. Nevertheless the structure is not always
easy to dissect free and may not be present in
some cases. Some authors resort to define the
ligament by internal rotation and sharp dissection
of a fold that appears in the deep soft tissue.
THE ILIOTIBIAL BAND AND
ITS ATTACHMENTS TO THE
DISTAL LATERAL FEMUR
It has been long realised that there are strong,
easily identifiable fibrous attachments from the
iliotibial band to the distal lateral femur. These
have been referred to as Kaplan’s fibres due to
the description in 1959 [8]. These lead into the
posterior portion of the iliotibial band described
by Terry as the deep capsulo-osseous layer [1].
The band of tissue thus formed from the fibres
attached to the femur pass distally within the
posterior iliotibial band to Gerdy’s tubercle
provide a thick, strong band of tissue that is
ideally located and aligned to resist internal
rotation of the tibia.
Having previously studied the ALL at
Imperial
College
[5] and described its anatomy our
research focus was on this structure. However
with further exploration of the lateral side of
the knee it became obvious that, not only was
the anterolateral ligament flimsy, but often hard
to find. In comparison the IT band and its
attachments to the lateral femur was present in
every knee and robust. We felt this worthy of
further study. The Kaplan’s fibres are arranged
in three specific attachments (retrograde, and
supracondylar attachments and proximal).
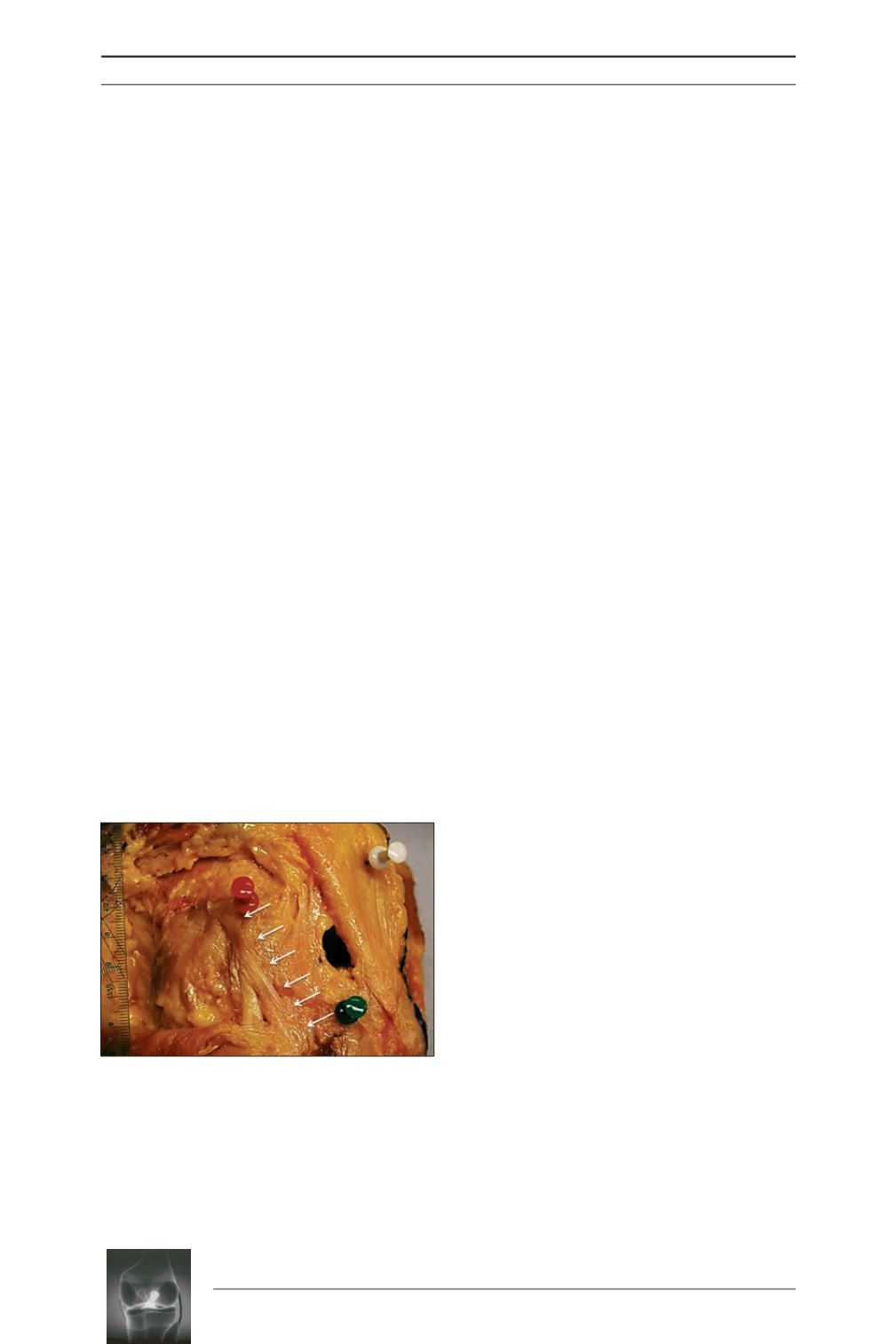
Fig. 1:
Dissection of a knee at 90 degrees flexion
demonstrating the anterolateral ligament.
Red
pin = femoral attachment of LCL;
green
pin =
Gerdy’s tubercle. The anterolateral ligament is
highlighted by white arrows, and is seen passing
obliquely superficial to the LCL from its femoral
attachment proximal and posterior to the femoral
LCL attachment, to the mid-point between the LCL
attachment to the fibula and Gerdy’s tubercle.
(Courtesy of Am J of Sports Med)
.