










 50 / 244
50 / 244

ANTEROLATERAL LIGAMENT OF THE KNEE
49
SURGICAL TECHNIQUE
We have previously described several ALL
reconstruction techniques that are performed
alone or in combination with ACL re
construction [19, 20]. The patient is placed in a
standard supine position with a lateral pad at
the tourniquet and a distal pad placed to keep
the knee at 90° intraoperatively.
Combined ACL/ALL reconstruction
[19]
We use the semitendinosus (ST) and gracilis
(G) tendons as grafts; they are harvested using
an open tendon stripper to preserve their tibial
attachment points. The ST is used to reconstruct
the ACL; it is tripled to provide a 12-cm long
graft from its tibial attachment. The gracilis is
then detached from its tibial insertion; one part
is used to quadruple the ST and its distal end is
used to reconstruct the ALL. This results in an
8-10mm diameter ACL graft. Two skin
incisions less than 1cm long are made to
prepare the ALL distal attachment sites: in front
of the fibular head and behind Gerdy’s tubercle
for the tibia. Next, two 4.5-mm connected
tunnels are made from these points to reproduce
the ALL’s tibial attachment. A third incision is
made at the femur, posterior and proximal to
the epicondyle. A suture is used to ensure that
the distance between these three points differs
when the knee is moved – the ALL must be
tight in extension and slack in flexion.
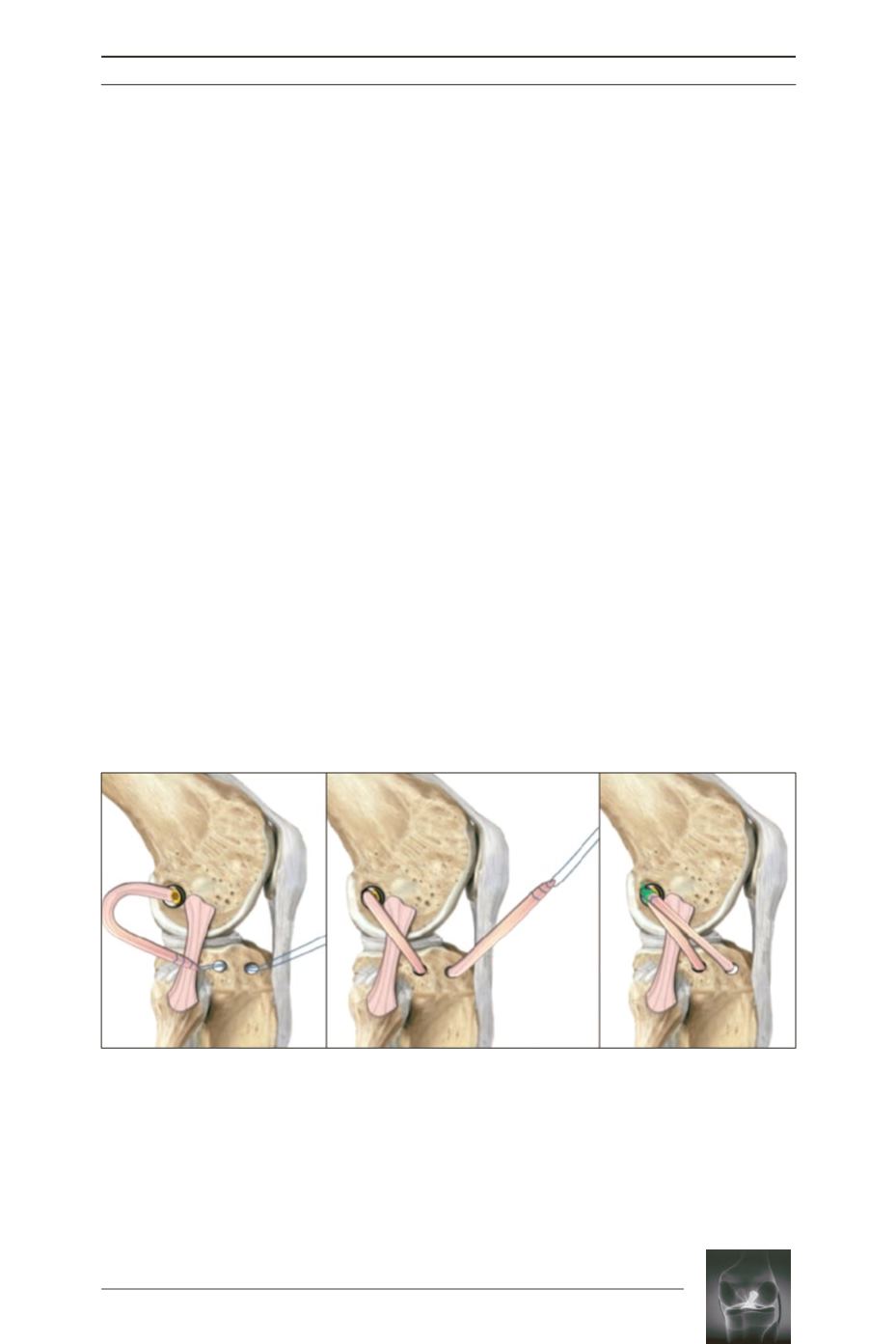
The ACL’s tibial tunnel is made in the standard
manner. Using an outside-in guide, the ACL’s
femoral tunnel is placed over the femur’s
isometric point (i.e. proximal to the epicondyle),
which corresponds to the ALL’s femoral
insertion. After passing the ACL graft from
inferior to superior, it is secured with
interference screws at the tibia and femur. The
pre-sutured gracilis strand is passed
subcutaneously and under the fascia lata, and
then retrieved through the superolateral
incision on the tibia; a traction suture is used to
pull it out of the anterior tibial tunnel. It is then
retrieved through the proximal incision over
the femoral tunnel and sutured to itself. With
the knee fully extended, this graft is secured
with an interference screw at the anterior tibial
tunnel to ensure it is tight in extension and
slack in flexion. The tibia must not be rotated.