










 181 / 460
181 / 460

S. Lippacher, H. Reichel, M. Nelitz
180
Materials and methods
Lateral radiographs and transverse MRI T2-
weighted scans of fifty knees in fifty patients
with patellar instability that were referred to
our outpatient-clinic between 2007 and 2010
for subsequent surgery were analyzed. None of
these patients had prior surgery of the knee.
Patients with insufficient X-ray or MRI were
excluded. In all included patients routine
X-rayswere taken to evaluate the patellofemoral
joint. The lateral view was taken in the supine
position and 0° knee flexion with superimposed
condyles [17]. During clinical assessment a
firm typing was made using the D. Dejour’s
classification.
This study compares the reliability and accuracy
of two diagnostic studies in grading the severity
of trochlear dysplasia.
The radiographic study (method 1) included a
correct plain lateral view of the knee.According
to D. Dejour [9] on lateral radiographs four
different types of trochlear dysplasia were
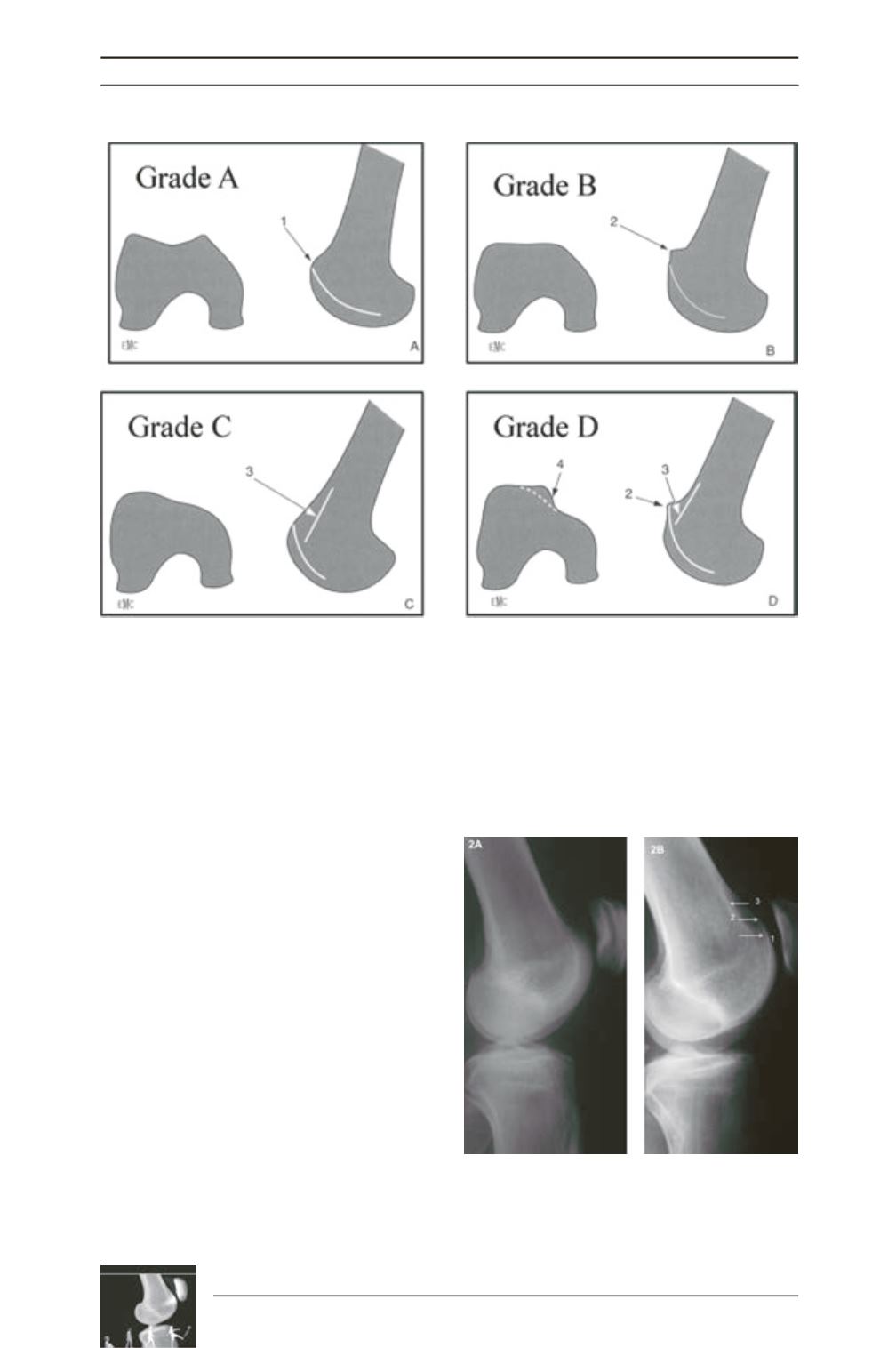
distinguished (fig. 1, 2).
Fig. 1: Classification of trochlear dysplasia according to D. Dejour (reprintedwith David Dejour’s permission):
1 – crossing sign, 2 – supratrochlear bump or spur, 3 – double contour, 4 – vertical join or cliff pattern.
Fig. 2:
A: Normal patellofemoral joint.
B: trochlear dysplasia with crossing sign (1), small
supratrochlear bump or spur (2), double contour