








 121 / 242
121 / 242

Lateral unicompartment knee arthroplasty (UKA)
121
Ligament balance
The principle of the UKR is to “slide” the
implant prosthesis into the ligamentous
envelope of the knee, which will fill the spaces
created by bone cuts (fig. 2).
Only loss bone space by wear must be corrected
(leaving a small hypocorrection).
Classically, during the UKR procedure, the
ligament releases are forbidden. However,
different scenarios could be presented:
- In case of reducible deformity
, ligament
release is non indicated. A subperiosteal
release of the capsule could be done.
- In case of partially reducible deformity
(small
ligament retraction) a limited well controlled
release can carefully done to avoid an
overcorrection by unilateral ligament
elongation and consequently a increase of
space (that must be filled by the increase of
the thikness of the polyethylène of UKR).
Tibial cut
(fig. 3A and 3B)
Different cases can be present in the lateral
femorotibial osteoarthritis :
• Constitutional valgus knee : the originated of
the valgus is on the femoral side, which is
usually produced by hypoplasia of the lateral
femoral condyle.
If the lateral femoral condyle (hypoplasia) is
the line of reference to define the height of
tibial cut, it will correct the femoral deformity
with a increasing of the tibial polyetilene
thickness.
If the thickness of a femoral component is
fixe it could promote a partial or total
correction of the deformity (by femoral
component thickness). On the other hand,
when the deformity is severe it could lead to:
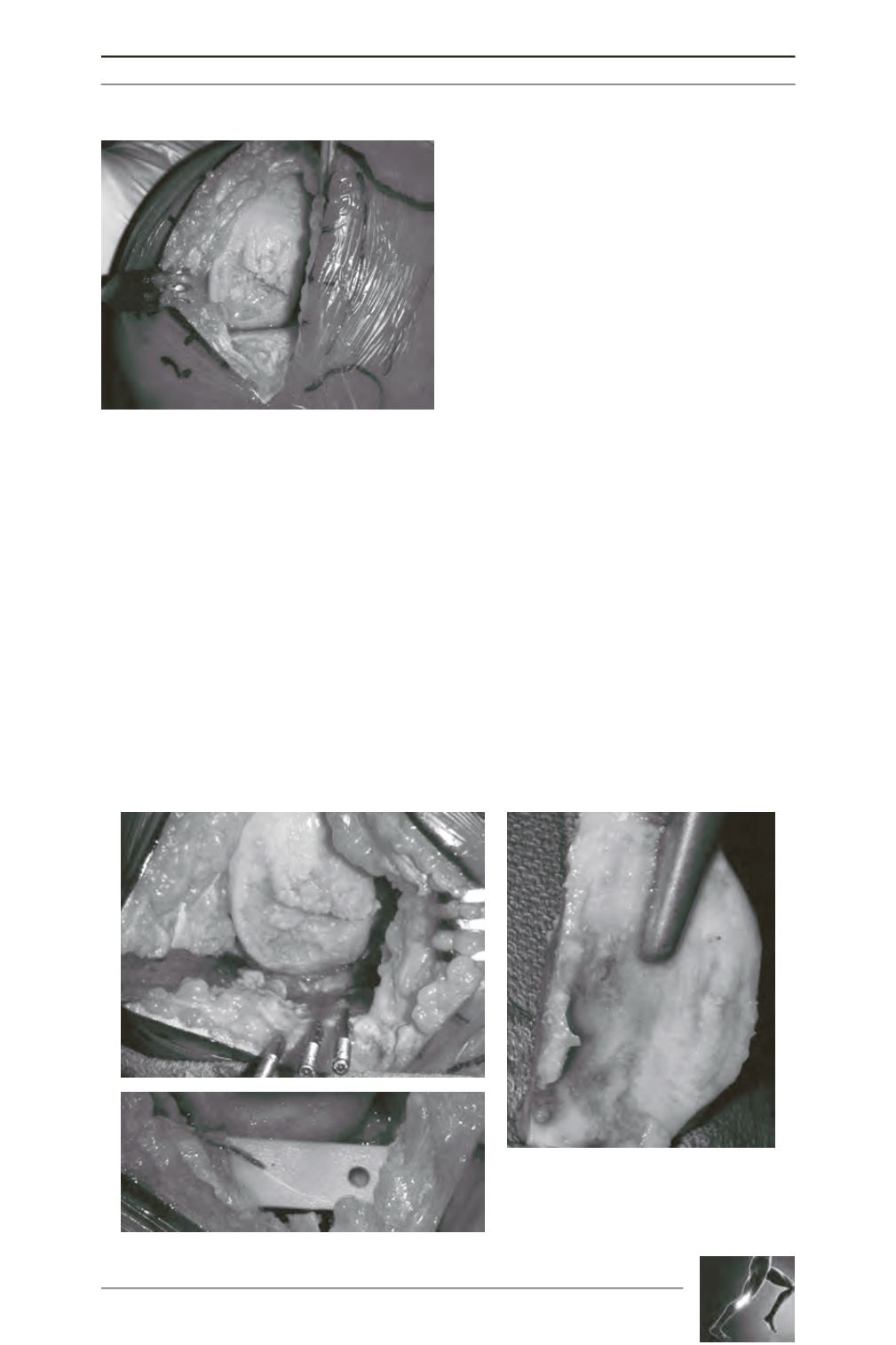
Fig. 1D: R Knee - Good exposition without patella
eversion and without quadriceps incision.
Fig. 2A at 2C - The goal of the UNI is to
adapt the frontal deformity of the knee.
The prosthesis must correct the wear
deformity of the tibia without changing
the envelope ligament.
A
C
B
D