








 122 / 242
122 / 242

R. Badet, S. Piedade
122
- polyethylene oversize and consequently, an
elevation of joint line;
- a persistent residual valgus deformity.
In such cases, we advise to use a resurfacing
UKR, because the thicknesses of the femoral
components vary, which help reconstruct the
lateral condyle and to restore to the adequate
level of the joint line (fig. 3C to 3E).
• After a fracture or a depression of the lateral
tibial plateau the origin of the valgus knee is
on the tibial side. The deformity and the wear
has been originated on the tibia and lateral
condyle which is “normal or with mild wear”
could be a reference to perform the tibial cut
with no risk of malpositioning or oversizing
of the tibial plateau component.
In theses cases there is a risk of hypercor
rection related to the thickness of the femoral
component and a resection prosthesis (“cut”)
UKR should be performed.
• In case of lateral femorotibial osteoarthritis
secondary to meniscetomy, the surgeon must
bear in mind that the origin of the valgus
deformity (femur or tibia) takes an important
role and should guide the surgical strategy.
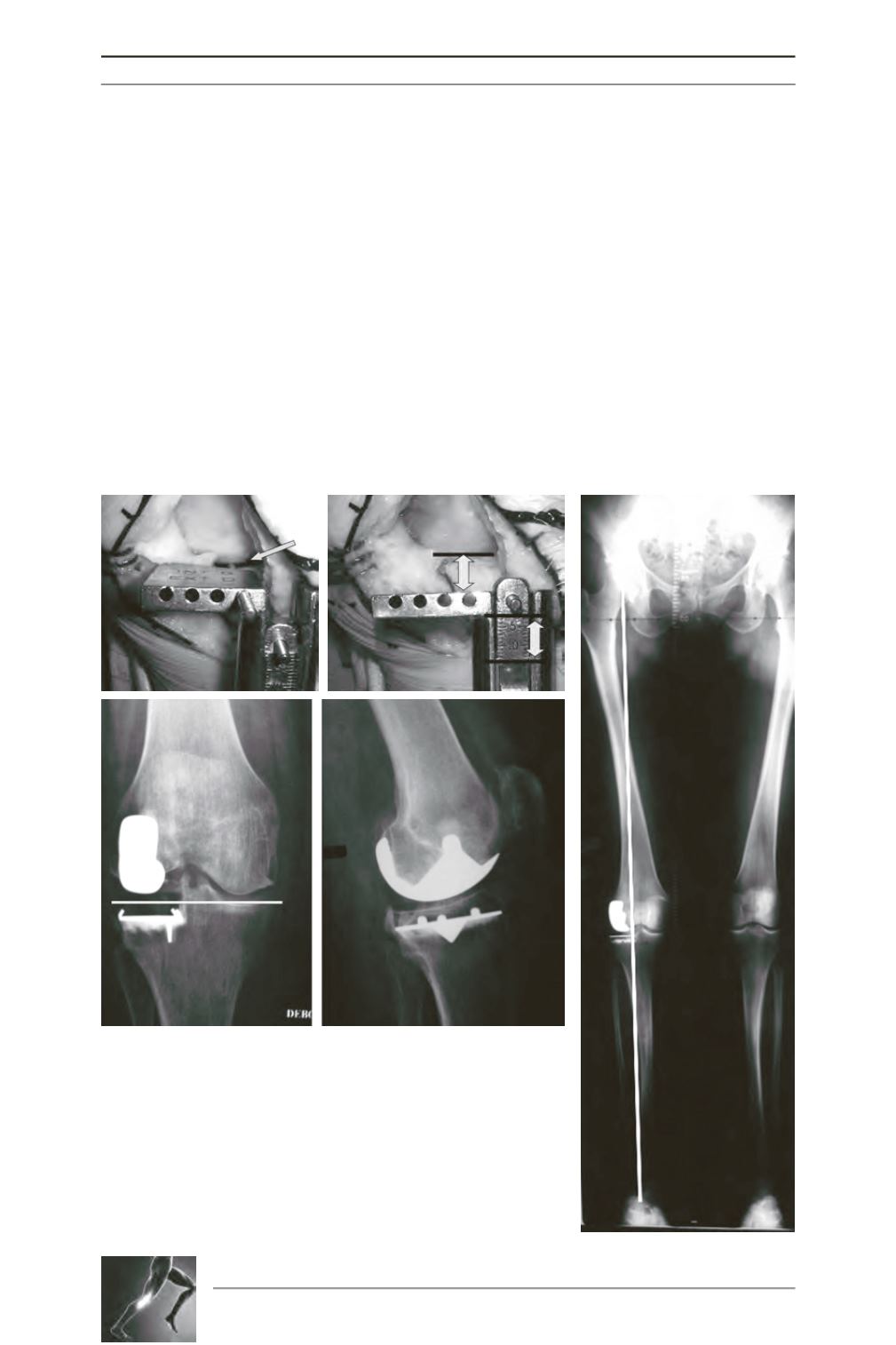
Fig. 3A: R Knee - Intra articular pin: We use a reference pin which is
insert in the femoro tibial worn compartment to check to control and
reproduct the patient’s tibial slope during the procedure.
To restore to the adequate level of the joint line.
Fig. 3B: R Knee - In this case: cut at 13mm under the lateral condyle:
- 3mm femoral condyle
- 9mm Tibial polyéthylène
- 1mm security laxity to avoid over correction
Fig. 3C at 3E - In such cases, we advise to use a resurfacing UKR,
because the thicknesses of the femoral components vary, which help
reconstruct the lateral condyle and to restore to the adequate level of
the joint line.
C
D
A
B
E