








 123 / 242
123 / 242

Lateral unicompartment knee arthroplasty (UKA)
123
Tibial Slope and tibial cut
Some systems have incorporate a fixed tibial
slope, while others promote an adaptation to
the patient’s tibial slope (constitutional tibial
slope, ACL fragility) in each case.
It should keep in mind that UKA is adapted to
the knee with no modification to ligamentous
envelope. It is important to adapt the tibial
slope of the prosthesis to the tibial slope of the
patient. In these case it is very important to use
a system with a variable valor of the tibial
slope. We use a reference pin which is insert in
the femoro tibial worn compartment to check
to control and reproduct the patient’s tibial
slope during the procedure (fig. 3A).
Coronal plane and tibial cut
The goal of the UNI is to adapt the frontal
deformity of the knee.
The prosthesis must correct the wear deformity
of the tibia without changing the envelope
ligament and must keep a slight hypo correction.
This necessarily requires to adapt the frontal
cut of the tibial cut at each case using a
extramedullary
reference
system
(the
intramedullary reference systems being
prohibited within the constraints of the surgical
approach and ACL respect).
Choise of the tibial implant
Whatever the type of prosthesis, the
implant should not overflow the tibia
bone. The tibial implant should be fixed
(mobile platforms are to be inadvisable in
the external UNI because of the risk of
polyethylene dislocation).
Femoral Cut
It requires the use of specific tool who are
positionned in inter-condylar notch to tract the
patella.
The femoral preparation is specific depending
on whether if it is a resurfacing prosthesis or if
it is cutting prosthesis.
Do not resect the external osteophytes before a
good positionning of the condylar implant.
Femoral implant positioning
(fig. 4a-4f)
The femoral implant must be positioned with a
control of the position in all planes:
- In the frontal plane
we recommend a
perpendicular position of the femoral implant
relative of the tibial plane (with 90° knee
flexion). This may result a position of the
condylar implant different than the condyle
axis (fig. 4a 4b), in particular on the lateral
condyle where the condylar implant can be
positionned on the latéral osteophytes.
- In the medio-lateral plane:
it is very important
to avoid conflict with the tibial spine in
positionant the femoral condyle as close to
the middle of the condyle sometimes on the
lateral edge of the lateral condyle.
- In the sagittal plane:
it is very important to
avoid “camber of condyle” which can lead
punctiform or a linear constraint of the
femoral implant on the tibial plateau, source
of polyethylene wear and degradation
(delamination and creep).
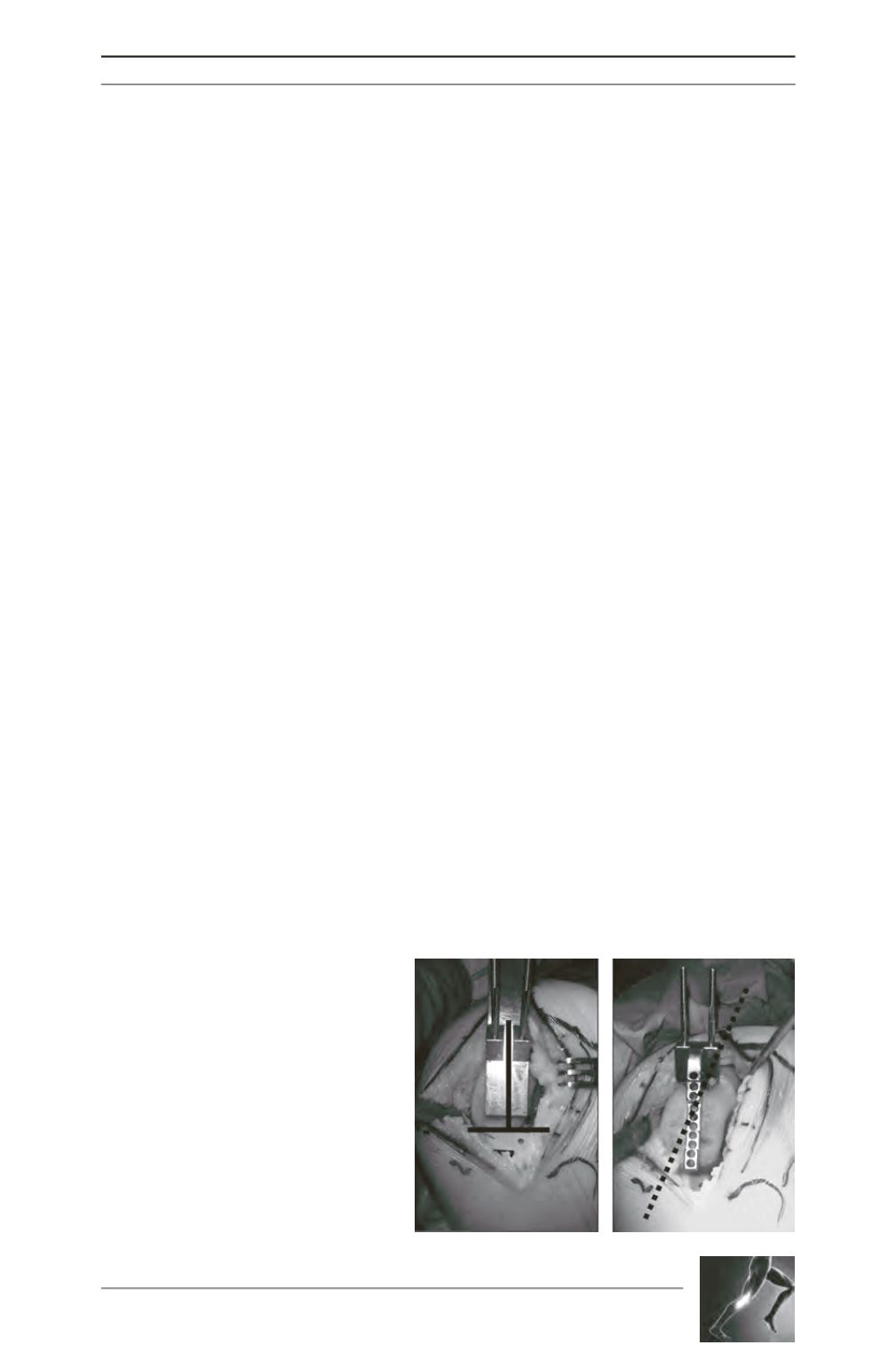
Fig. 4A and 4B - In the frontal plane we
recommend a perpendicular position of the
femoral implant relative of the tibial plane
(with 90° knee flexion). This may result a
position of the condylar implant different than
the condyle axis, in particular on the lateral
condyle where the condylar implant can be
positionned on the latéral osteophytes.
A
B