








 134 / 242
134 / 242

R.A. Magnussen, S. Gunst, V. Villa, C. Debette, O. Reynaud, E. Servien, S. Lustig, P. Neyret
134
Discussion and
conclusion
The main finding of this study was both the
medial and lateral parapatellar approaches
resulted in similar, good results following TKA
in knees with mild valgus.
The achievement of a balanced knee may be
more difficult in cases of valgus deformity than
in knees with standard varus osteoarthritis,
possibly resulting in excessive releases of
lateral structures. The main theoretical
advantage of the lateral approach is a better
visualization, and a preservation of these tight
lateral tissues [7]. Previous studies have
demonstrated a 20-fold increased risk of
revision if both the collateral lateral ligament
and the popliteus tendon are released [5].
Sekiya
et al.
found a tendency toward fewer
release in their lateral approach group [8],
suggesting that a capsular release is enough in
most cases when performing a lateral approach.
The lateral approach also avoids patellar
devascularization that can occur when a lateral
retinacular release is performed in the setting
of a medial parapatellar arthrotomy [3]. The
increased postoperative range of motion noted
by Sekiya
et al.
with the lateral approach [8]
was not demonstrated in our series, possibly
due to a lower preoperative valgus deformity
(6°) compared to Sekiya
et al.
(13°). The lateral
approach may also result in improved patellar
tracking in some patients following TKA [2].
The lateral approach may be more efficient in
restoring lower limb alignment as suggested by
Apostolopoulos [1, 6], particularly in patients
with a large valgus deviation. We did not find
any difference in the post-operative mechanical
axis in our series of moderate valgus, which is
consistent with the results of Sekiya
et al.
[8].
For many authors, the lateral approach is not
familiar technique to perform, and is considered
to be technically more difficult than the medial
approach. This expectation is due to the
presumed necessity of performing an associated
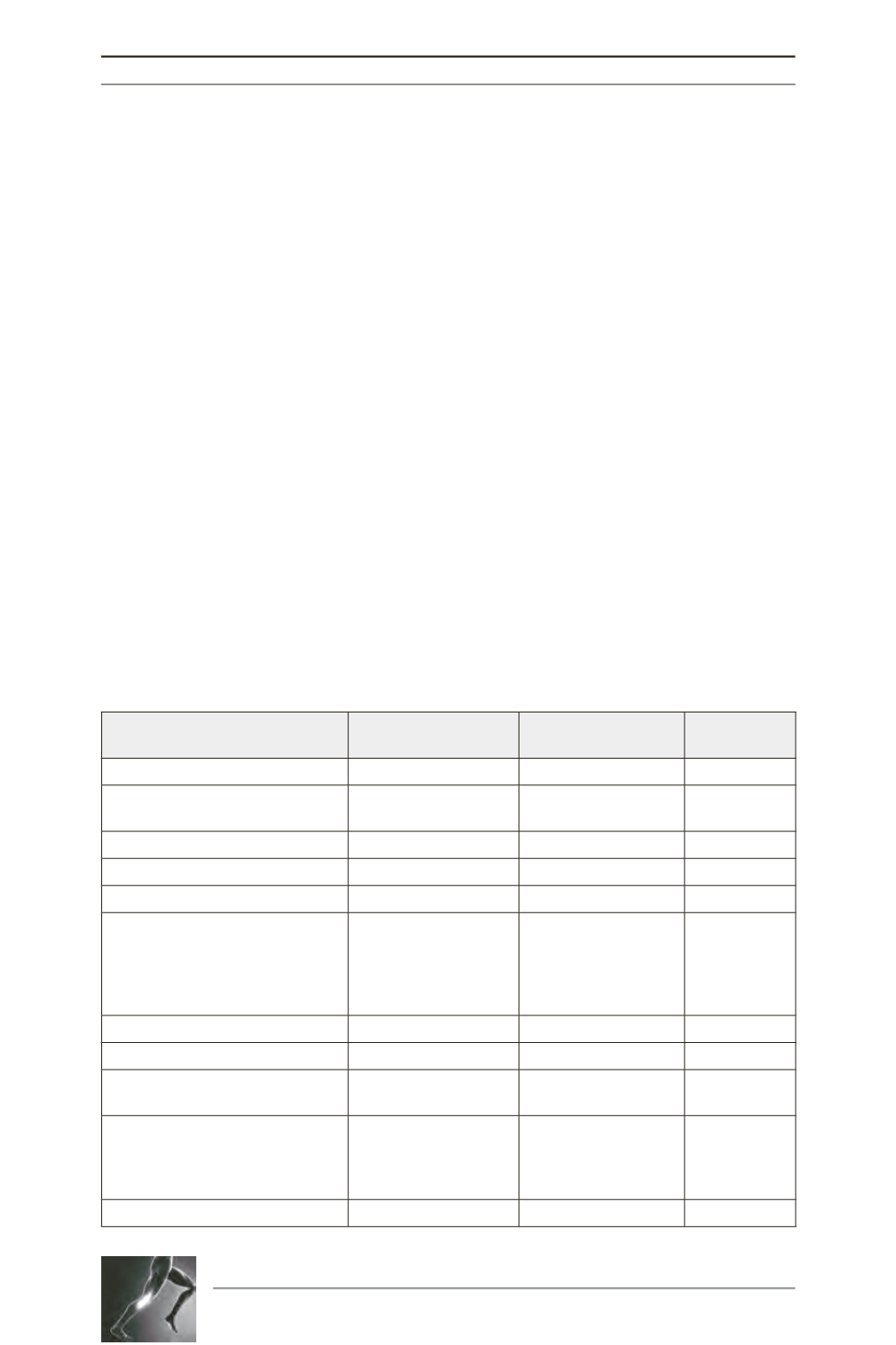
Table 1 - Pre-operative Data
Lateral Approach
n = 315
Medial Approach
n = 109
Significance
Age (years)
70.9 ± 9.4
68.1 ± 11.2
p = 0.020
Sex
Male = 60 (19.1%)
Female = 255 (80.9%)
Male = 24 (22.0%)
Female = 85 (78.0%)
p = 0.49
Weight (kg)
74.9 ± 12.7
71.2 ± 16.3
p = 0.029
BMI (kg/m
2
)
27.6 ± 4.3
26.4 ± 5.2
p = 0.030
Prior open knee surgery
51 (16.2%)
15 (13.8%)
p = 0.33
OA Grade
. Grade 1
. Grade 2
. Grade 3
. Grade 4
5 (2.0%)
68 (27.2%)
122 (49.2%)
53 (21.4%)
2 (3.4%)
21 (35.6%)
24 (40.7%)
12 (20.3%)
p = 0.45
IKS Knee Score
51.8 ± 15.6
47.1 ± 18.2
p = 0.017
IKC Function Score
57.4 ± 18.7
52.1 ± 20.7
p = 0.019
Flexion contracture of 5 deg
or greater
100 (31.7%)
39 (35.8%)
p = 0.48
Alignment
.
HKAA (degrees)
. FMA (degrees)
. TMA (degrees)
186.6 ± 2.3
93.7 ± 3.0
90.4 ± 2.8
185.4 ± 2.3
93.1 ± 3.4
89.4 ± 3.4
p < 0.0001
p = 0.10
p = 0.0064
Blakburne-Peel Index
0.84 ± 0.23
0.77 ± 0.17
p = 0.001