








 138 / 242
138 / 242

D. Beverland, E. Doran, S. O’Brien, J. Hill, R. Pagoti
138
groove. In knees with a Sperner Grade 4
deformity of the patella [2] “patella contouring”
(removal of the abnormal traction osteophyte)
is performed (fig. 3). Postoperatively the knee
is immobilised at 90 degrees flexion for six
hours. We believe this reduces the risk of
peroneal nerve injury and we have also shown
that it reduces blood loss [3].
All components were cementless, except in
14 patients (2.6%) where bone was considered
poor and cement was used on the tibial side [4].
However in the last five years no cemented
component has been used. When using a
cementless tibial tray care should be taken to
use autologous bone graft in any areas of soft
and then ensure that during impaction the tibial
tray descends evenly from medial to lateral and
anterior to posterior.
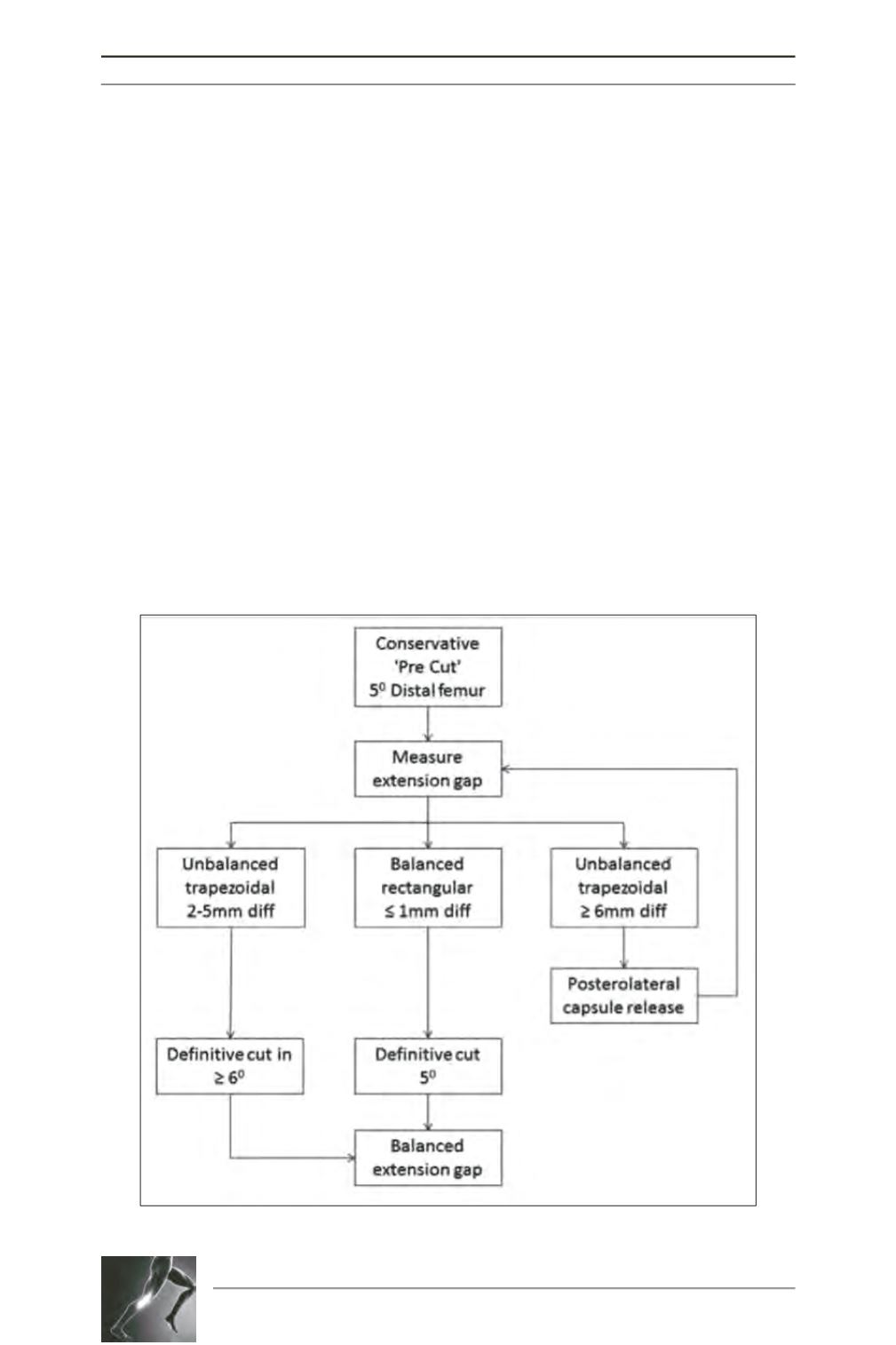
When using this technique with a pre-operative
valgus deformity of ≥10 degrees approximately
70% of patients have a release of the postero-
lateral capsule either with or without a definitive
cut of ≥6 degrees, a further 20% just have a
definitive cut of ≥6 degrees and 10% have a
definitive cut of 5 degrees. The IT band was
released in 16 patients (3%) but this was only
in the earlier part of this series. We no longer
release the IT band.
Lateral patellar release was performed in
75 knees (14%) and 45 knees (8.3%) had
patellar contouring. The incidence of lateral
patellar release in knees ≥200 deformity was
twice that of knees with 10-190 deformity.
(24.5% vs. 11.7%) (Fisher’s exact test the
p
-value is 0.026). This compares to a 4% lateral
patellar release in our varus knees.
Fig. 1: Algorithm to balance the extension gap in valgus knees.