








 81 / 242
81 / 242

The reasons for a customized knee prosthesis Stepping outside the Square
81
has been questioned as to whether it is essential
to prevent failure [32], and it is not necessarily
associated with better functional outcomes [33-
36]. Some authors have promoted the
restoration of a given degree of native
deformity, especially when from femoral
origin, along with the original joint line
obliquity [37-42]. This concept may be
reinforced by studies utilising CAS which have
resulted in more accurate ‘traditionally’ aligned
prostheses but without demonstrating superior
functional outcomes [43, 44].
Moving closer to natural alignment may also
be tolerated as improved prosthetic materials
may tolerate variations in alignment in terms of
wear rate [45].
The ideal rotational alignment is still the subject
of controversy [46], and may be seen as a
palliative attempt to offset an asymmetrical
flexion gap and/or to make-up a poor patellar
pace [47, 48].
The recent advances in
Prosthetic design
Femoral Sizing and Shape
Independent from alignment factors affecting
outcome, several publications have pointed out
prosthetic design limitations regarding; sizing,
AP/ML mismatch, and trochlear design [49].
AP sizing of the femur is dependent upon
individual femoral anatomy and the degree of
rotation and flexion of the femoral component
chosen by the surgeon [50]. Selection of
implant sizes between surgeons is variable
depending on experience and philosophy [51],
Overhang of the femoral component is highly
prevalent, occurring frequently and with greater
severity in women. Overhang also increases as
larger femoral component sizes are used in
both sexes. Femoral component overhang can
double the risk of long term knee pain [52, 53]
and lead to worse flexion and function [53].
Aside from overhang, the cut surface of the
femur is often not covered adequately by the
definitive prosthesis, leaving sharp edges on
which the soft tissue envelope abuts (fig. 2 & 3).
As a result, the most recently released
prostheses are showing an increasing number
of sizes across the range – extreme sizes being
delivered on demand – with optional narrower
femoral components and extended options to
allow femoral and tibial dissociation (Table 1).
However significant increases of shear strain
occurs in the peripheral proximal regions of the
tibia when loaded with a larger versus a smaller
femoral component, indicating the importance
of a correct sizing relationship [54].
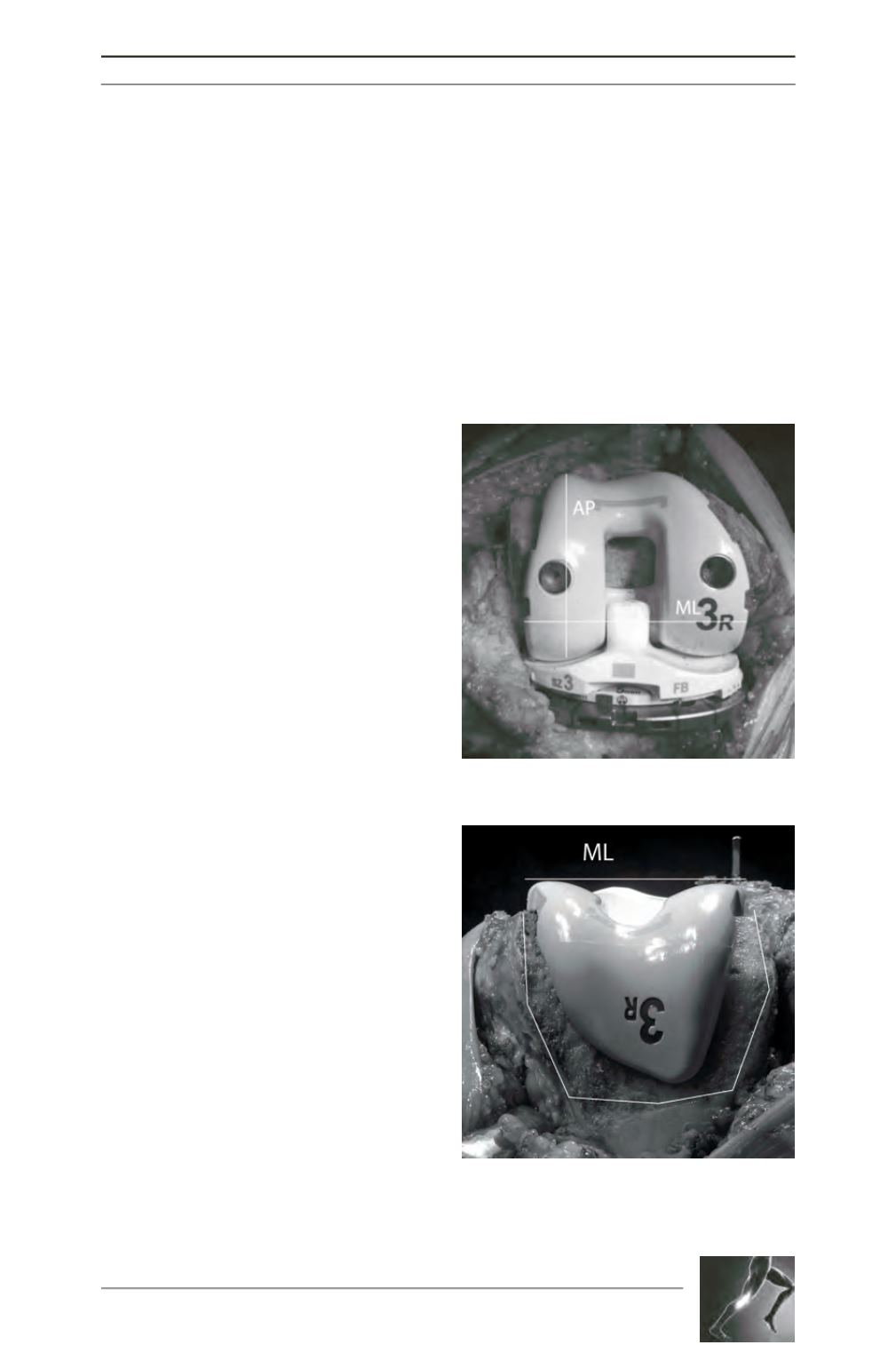
Fig. 3: Superior view of the same patient (figure 2)
showing a lack of the trochlear coverage and
subsequent sharp edges, despite perfect AP/ML
dimensioning.
Fig. 2: Perfect AP/ML dimensioning in a female’s
right knee with a modern design implant.