








 76 / 242
76 / 242

M. Bonnin
76
Conclusion
To our kowledge, this is the first investigation,
which analyses the relationships between
implants and soft tissues after TKAs’. This
work demonstrates that the optimal sizing in
TKA is very challenging due to the non-
anatomic design of current implants. The main
finding is that surgeons must analyse sizing in
term of volume rather than in term of surface.
In other words, most apparently “normosized”
TKA, in term of surface coverage are in fact
oversized in term of prosthetic volume.
Therefore, with current implants we should
aim at undersizing our implants, both in the
mediolateral dimension (Femur & Tibia) and
in the anteroposterior dimension (Tibia).
Anteroposterior sizing of the femur is more
complex because it may influence ligament
balancing in flexion and at mid-flexion. At the
anterior aspect of the femur (from overhang of
the trochlea to anterior notching) malsizing can
be a cause of anterior pain due to impingement
with the Patellofemoral ligaments and with the
anterior capsule. At the posterior aspect of the
femur inadequate posterior condyle resection
may compromises the results due to excessive
ligament tension or laxity. Therefore,
anteroposterior sizing at the femur is not purely
dictated by anatomic considerations.
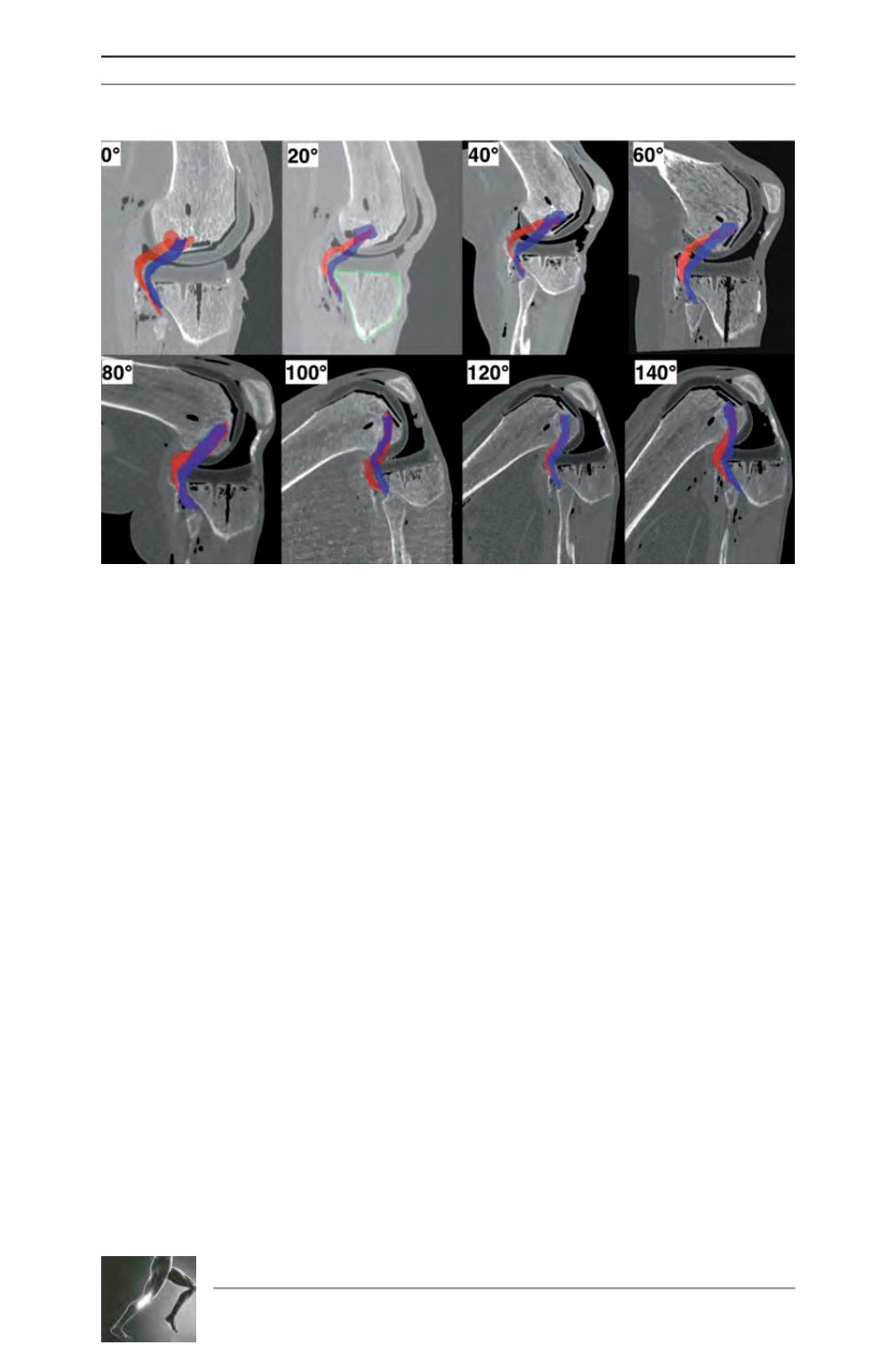
Fig. 6: On this specimen, an intentionally oversized TKA was implanted. The position of the PT before
implantation (blue) and after implantation (red) are suprimposed. The tracking of the PT is obviously
modified by the tibial plateau.