








 98 / 242
98 / 242

F. Lavoie, K. Iguer, F. Al-Shakfa
98
identical rectangular extension and flexion
gaps, similar to the original technique of
Cloutier, however the surgical flow is smoother
and operative times are comparable to other
knee arthroplasty techniques.
Clinical results
The first 100 bicruciate-retaining TKAs
performed with this implant and the revisited
technique
(Hermes 2C, Ceraver Osteal,
Roissy, France)
by the first author were
reviewed. A cohort of 100 posterior-stabilized
TKA
(Hermes PS, Ceraver Osteal, Roissy,
France)
matched for sex and height with the
bicruciate-retaining arthroplasty cohort also
performed by the first author was also reviewed
as well (Table 1). The shape of the femoral
component of the two implants is essentially
identical, other than the intercondylar portion;
both implants offer essentially no rotational
constraint in the transverse plane; finally the
surgical technique for the two cohorts is the
same, other than the preservation of the
cruciate ligaments: it is therefore reasonable
to think that this comparative study, although
far from perfect, can provide some insight on
the impact of preserving both cruciate
ligaments during TKA.
Our results confirm that bicruciate-retaining
TKA results in good clinical outcomes with
significant improvement of the two components
of the Knee Society (KS) score and of all five
components of the KOOS (Table 2). Knee
instability was not an issue for the two cohorts,
most probably because of the surgical technique
that was used. However, like Goutallier
et al.
[6], we observed a decrease in maximal knee
flexion at the last follow-up. In our series, the
2C knees lost an average of 8 degrees of flexion
compared to the pre-operative value, while the
PS knees gained an average of 5 degrees of
flexion. Also, five patients with a bicruciate-
retaining prosthesis had a mobilization of their
knee under general anesthesia compared to
none in the posterior-stabilized cohort.
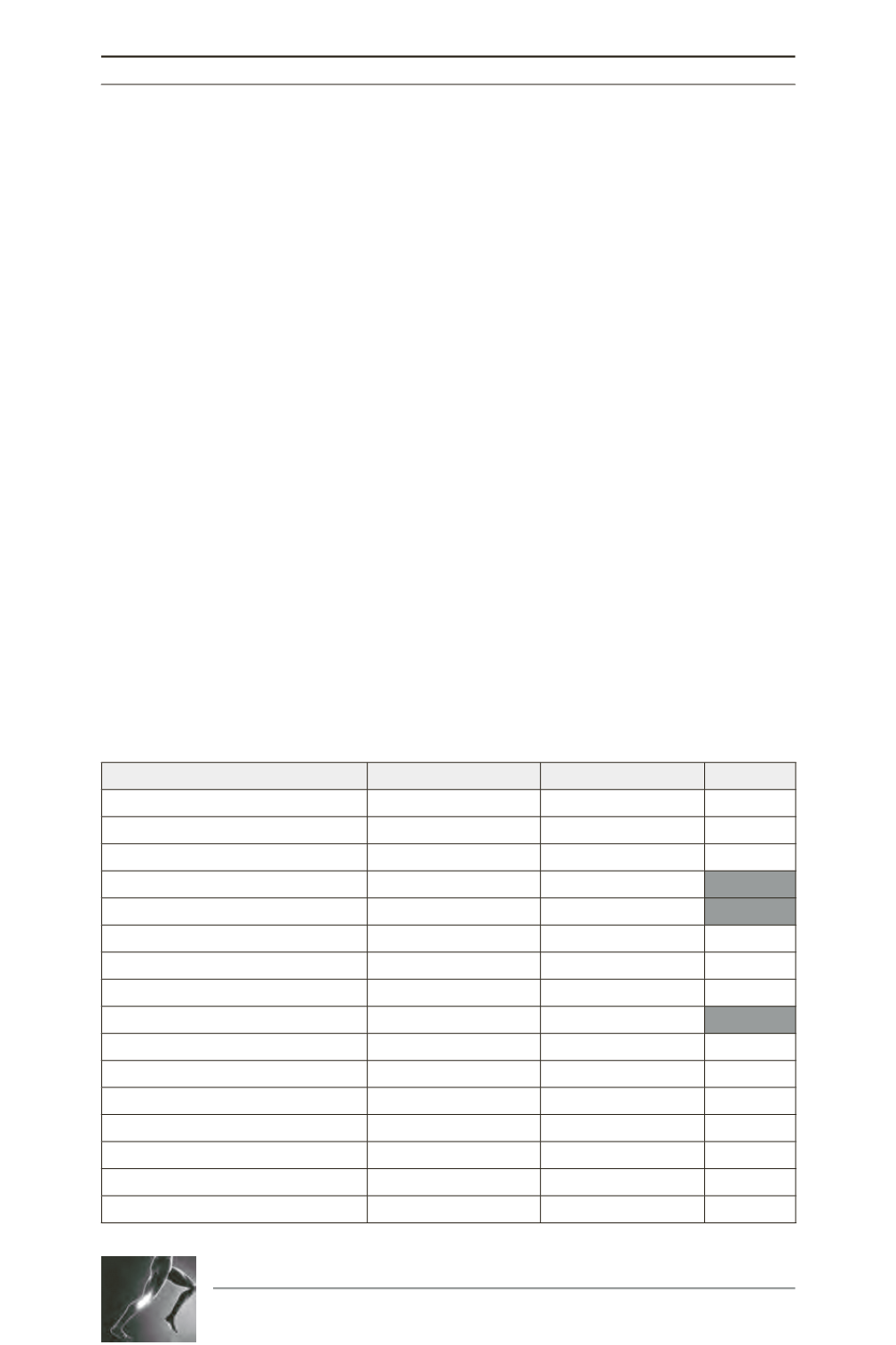
Table 1: Pre-operative data for Bicruciate-retaining (2C) and Posterior-stabilized (PS) TKA cohorts.
2C
PS
p value
Number of knees
100
100
Number of patients
90
88
Male/Female
37/63
34/66
0,658
Age (range)
63 (45-83)
67 (43-85)
0,002
Weight (kg)
89,5
81,3
0,003
Height (m)
1,65
1,65
0,687
Medial HKA angle (range)
174,5 (163-191)
174,3 (153-194)
0,807
Knee flexion contracture (range)
1,3 (0-15)
2,4 (0-20)
0,051
Knee flexion (range)
127,2 (100-160)
119,8 (40-160)
0,030
KS Knee Score
48,7
44,1
0,089
KS Function Score
56,6
53,5
0,262
KOOS - Pain
33,4
35,3
0,500
KOOS - Symptom
39,1
40,6
0,613
KOOS - Activities of daily life
38,0
37,6
0,875
KOOS - Sporting activities
12,0
11,9
0,972
KOOS - Quality of life
20,6
22,3
0,560