










 132 / 244
132 / 244

REPAIR OF MENISCAL RAMP LESIONS THROUGH A POSTEROMEDIAL PORTAL DURING ACL RECONSTRUCTION…
131
Rehabilitation
Postoperatively, the active and passive range of
motion is limited to 0-90° in the first six weeks
and progression to full weight bearing by
postoperative week 3. Jogging is permitted
after week 12, pivot activity at 6 months, and
full activity at 9 months for all patients.
Evaluation Methods
Follow-up assessments were made using both
subjective and objective means. An
experienced sports medicine fellow performed
all the postoperative examinations. Patients
were divided into two groups: those with a
limited tear of the posterior segment (n=81)
and those with a tear which extends to the
midportion of the meniscus (n=51) that
required an additional repair through standard
anterior portal with meniscal suture anchor
and/or an outside-in suture. Using Barrett’s
criteria [12] a repaired meniscus was
considered healed if there was no joint-line
tenderness or effusion, and a negative
McMurray’s test at the latest follow-up. Knee
laxity was measured with the rolimeter
Arthrometer (Aircast, Boca Raton, FL)
postoperatively and knee function in activities
of daily living and in recreational and
competitive sports was assessed using the
Tegner and subjective IKDC scores
preoperatively and at last follow up [13].
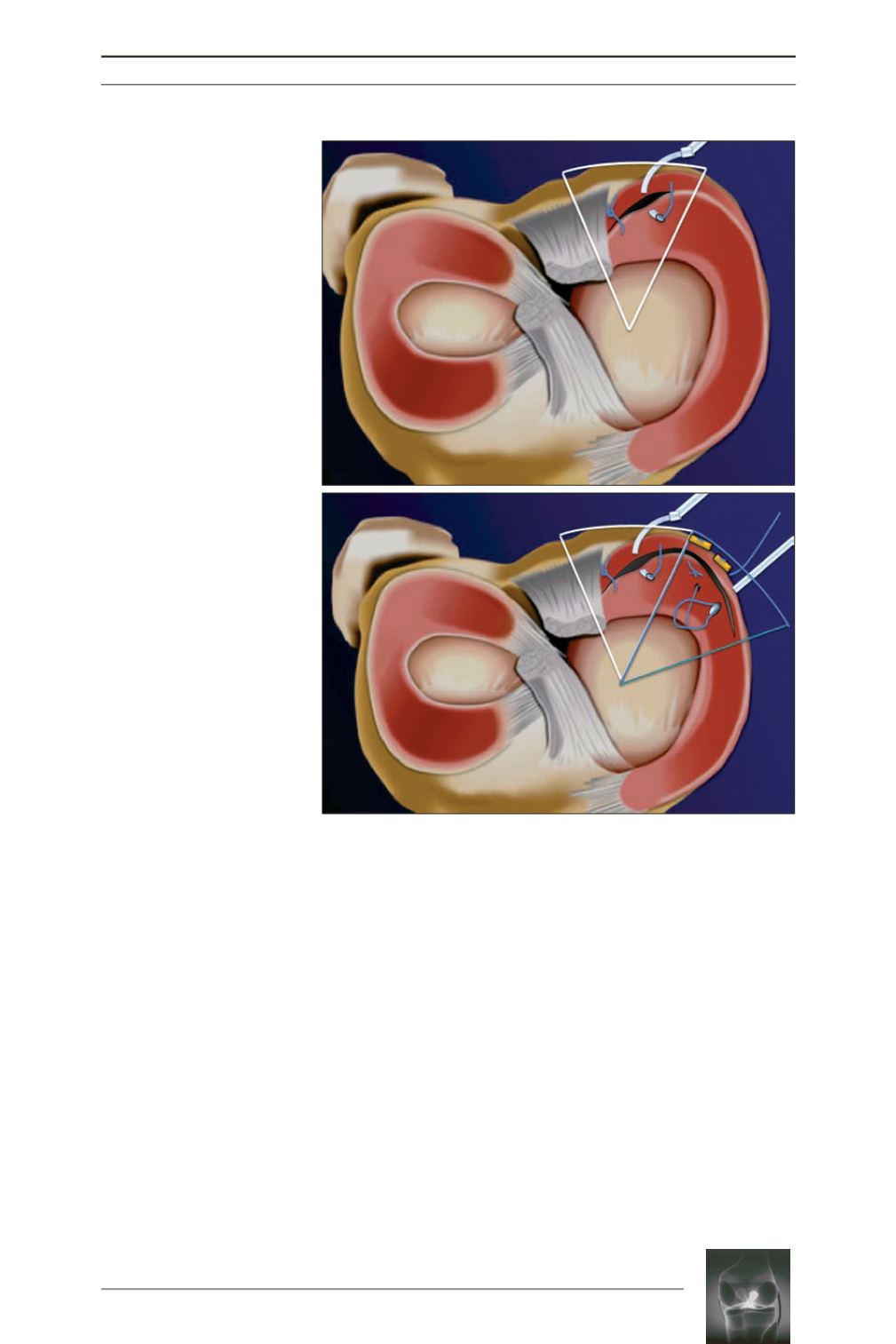
Fig. 3: a:
The posterior suture
is repeated as required
depending on the length of the
tear (one knot was inserted
every 5mm for tears limited to
the posterior segment (“limited
tears”).
b:
The posterior suture is
completedwith a repair through
standard anterior portal with a
meniscal suture anchor when
the tear extends to the pars
intermedia and/or by Outside-
In sutures (“extended tears).
a
b