










 141 / 244
141 / 244

C.H. BROWN
140
Anatomic ACLR is facilitated by using a
3 portal technique. The 3 portal technique is
versatile and can be used when performing
an anatomic ACL reconstruction with any
type of ACL graft and most fixation methods.
The 3 portal technique can be used for any
primary, revision, single- or double-bundle
ACL reconstruction. The technique is parti
cularly useful in cases where only one of the
two ACL bundles is torn or there is a large
remnant of the native ACL present. In these
situations, an augmentation or tissue pre
serving procedure can be performed.
Augmentation and tissue preserving proce
dures cannot be performing using a transtibial
or an all-inside technique.
In the 3 portal technique, the AL and AM
portals are used as viewing portals and the ACL
femoral tunnel is drilled through an accessory
anteromedial (AAM) portal. There are several
advantages of the 3 portal technique compared
to the traditional 2 portal approach:
• The 3 portal technique allows the surgeon to
interchange the working and viewing portals
according to the specific task that is being
performed;
• In the 3 portal technique, the lateral wall of
the intercondylar notch can be viewed
orthogonally through the AM portal while the
AAM portal is used as a working portal for
instrumentation. This approach allows the
surgeon to look and work in the same
direction, making it easier to achieve more
consistent and accurate placement of the ACL
femoral tunnel within the native ACL femoral
attachment site;
• Viewing the lateral wall of the intercondylar
notch through the AM portal also eliminates
the need to perform a notchplasty for
visualization purposes;
• Drilling the ACL femoral tunnel through the
AAM portal increases the obliquity of the
ACL femoral tunnel relative to lateral wall of
the intercondylar notch, resulting in a longer
femoral tunnel.
ARTHROSCOPIC PORTALS
• AL portal is created as close as possible to the
lateral border of the patellar tendon at the
height of the inferior pole of the patella;
• AM portal is created under arthroscopic
control at the height or slightly higher than
the inferior pole of the patella. An 18 gauge
spinal needle is passed into the knee joint
medial to the medial border of the patellar
tendon and directed toward the roof of the
intercondylar notch. The height of the spinal
needle is adjusted such that the shaft of the
spinal needle comes to lie parallel to the roof
of the intercondylar notch. This step results in
the external position of the spinal needle
being located proximal to the inferior pole of
the patella. Placing the AM portal at this
location ensures adequate spatial separation
between the viewing AM and the working
AAM portal. Due to the curvature of the
inferior pole of the patella, moving the AM
portal more medially makes it is possible to
achieve a higher AM portal position, creating
greater separation between the AM and AAM
portals (fig. 2).
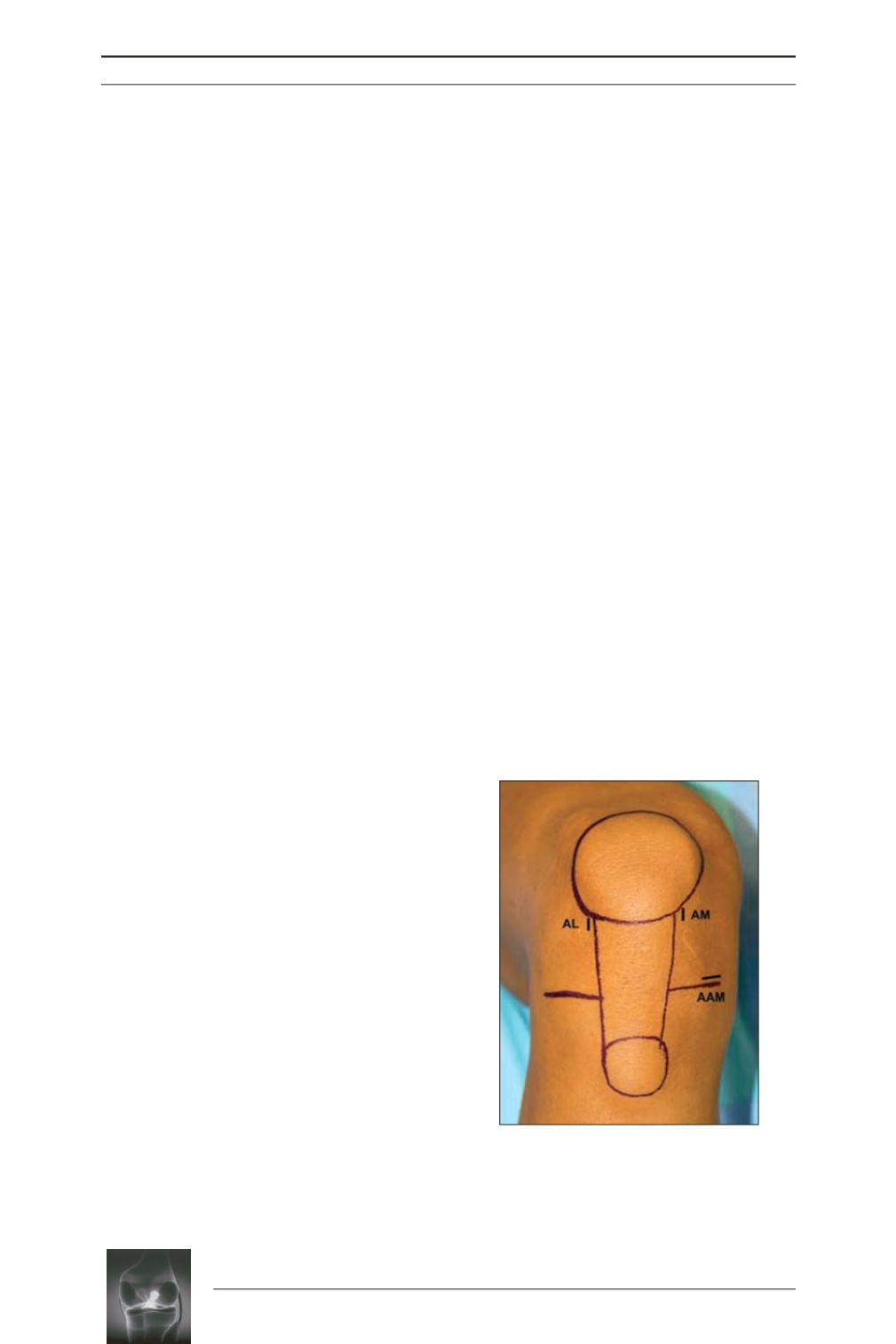
Fig. 2:
Surface landmarks and arthro
scopic portals: anterolateral portal (AL),
anteromedial portal (AM), accessory
anteromedial portal (AAM).