










 16 / 244
16 / 244

ANTEROLATERAL LIGAMENT HISTORY AND SURGICAL TECHNIQUES
15
Terry observed that increasingly abdnormal
Lachman test, pivot-shift test, and anterior drawer
at 90° of flexion afterACL rupture was correlated
with the integrity of the capsulo-osseous insertion
of the ITB [6]. This structure refers probably to
the ALL. Although the anterolateral structure is
incompletely understood; its function on
rotational control is undeniable. The majority of
sectioning studies reported an increased internal
rotatory laxity after the anterolateral capsule
section in ACL deficient knee, particularly at
flexion angles greater than 35°.
Claes have described another capsular structure
(fig. 2), whose the femoral attachment is
located on the prominence of the lateral femoral
epicondyle (LFE), anterior to the fibular
collateral ligament (FCL) attachment, proximal
and posterior to the insertion of the popliteus
tendon. Its distal insertion is on the anterolateral
proximal tibia, mid-way between Gerdy’s
tubercle and the fibular head, with no
connecting fibers to the ITB [7].
Another more superficial lateral structure has
been reported by Kennedy in 2015 [8]. Its
femoral attachment was on average 2.8mm
posterior and 2.7mm proximal to the FCL
attachment. Its distal insertion was on the
anterolateral tibia, posterior to Gerdy’s tubercle
(fig. 3). Their mechanical properties are still
poorly understood. Some reservations were
expressed on the role of this ALL [9] and thus
on its anatomic reconstruction.
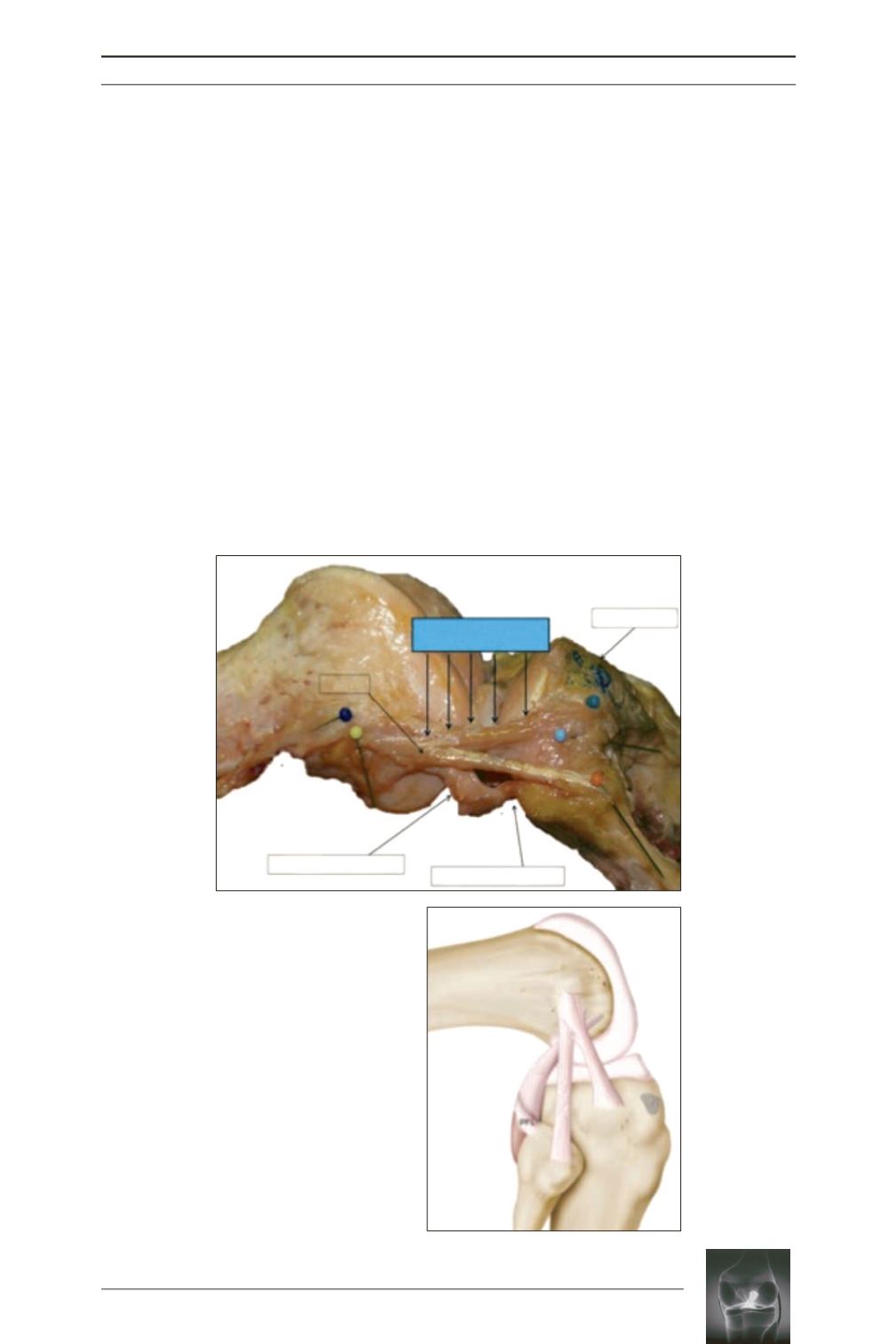
Fig. 2:
Cadaveric dissection
(a) and line drawing of a right
knee (b) showing the ALL
described by Claes
(from
Claes and al. [7])
.
ALL, anterolateral ligament; LCL,
lateral collateral ligament; LFE,
lateral femoral epicondyle; PT,
popliteus tendon; GT, Gerdy’s
tubercle.
b
a
Popliteus Tendon
LCL
Anterolateral Ligament
(ALL)
Gerdy’s Tubercle
LFE
PT
LCL
ALL GT
Popliteofibular Ligament