










 20 / 244
20 / 244

ANTEROLATERAL LIGAMENT HISTORY AND SURGICAL TECHNIQUES
19
A variation of this procedure has been
developed. A band of fascia lata (10cm by
10mm) is harvested and left attached on Gerdy’s
tubercle. This graft is passed underneath the
FCL, then in femoral tunnel with the bone
block of patellar tendon of intra-articular
reconstruction. The fascia lata graft is tensioned
at 30° of flexion in neutral external rotation of
the knee while the wedge shaped patellar bone
block is impacted into the femoral tunnel.
Marcacci technique
[24]
In this procedure, the gracilis and the semi
tendinosus tendons are harvested and sutured to
one another. They are left attached on the tibia,
and are passed through the tibial tunnel of ACL
reconstruction, then through the “over the top”
of the lateral femoral condyle. At the exit of the
femoral tunnel, they passed under the ITB but
superficial to the FCL, and then are fixed on
Gerdy’s tubercle by two staples at 90° of flexion.
“Anatomic” anterolateral ligament
reconstructions
Currently other surgical techniques called
“anatomic” have been described. Their aim is
to reproduce the insertion sites of the more
superficial ALL, described by Kennedy [8].
They are recent and few results are reported.
The Smith technique [25] consists of an “all
inside” ACL reconstruction with the
semitendinosus tendon, associated with an
independent extra-articular reconstruction with
the gracilis tendon. Two bone tunnels are
drilled: the first just anterior and superior to the
FCL femoral insertion and the second halfway
between Gerdy’s tubercle and the fibular head.
The gracilis tendon is fixed into the femoral
tunnel with threaded knotless anchor, and then
it is passed under the ITB and is fixed into tibial
tunnel with anchor.
CONCLUSION
Various techniques are performed to control
rotational stability with ACL deficient. They
are based on different principles: anterolateral
extra-articular augmentation or anatomic ALL
reconstruction. The different studies reported
satisfying results for the combined extra and
intra-articular reconstructions. However few
studies compared the various extra-articular
procedures. The “anatomic” reconstructions
are recent and should be evaluated at long term.
The mechanical properties and the function of
this superficial ALL are still poorly understood
and need more investigations.
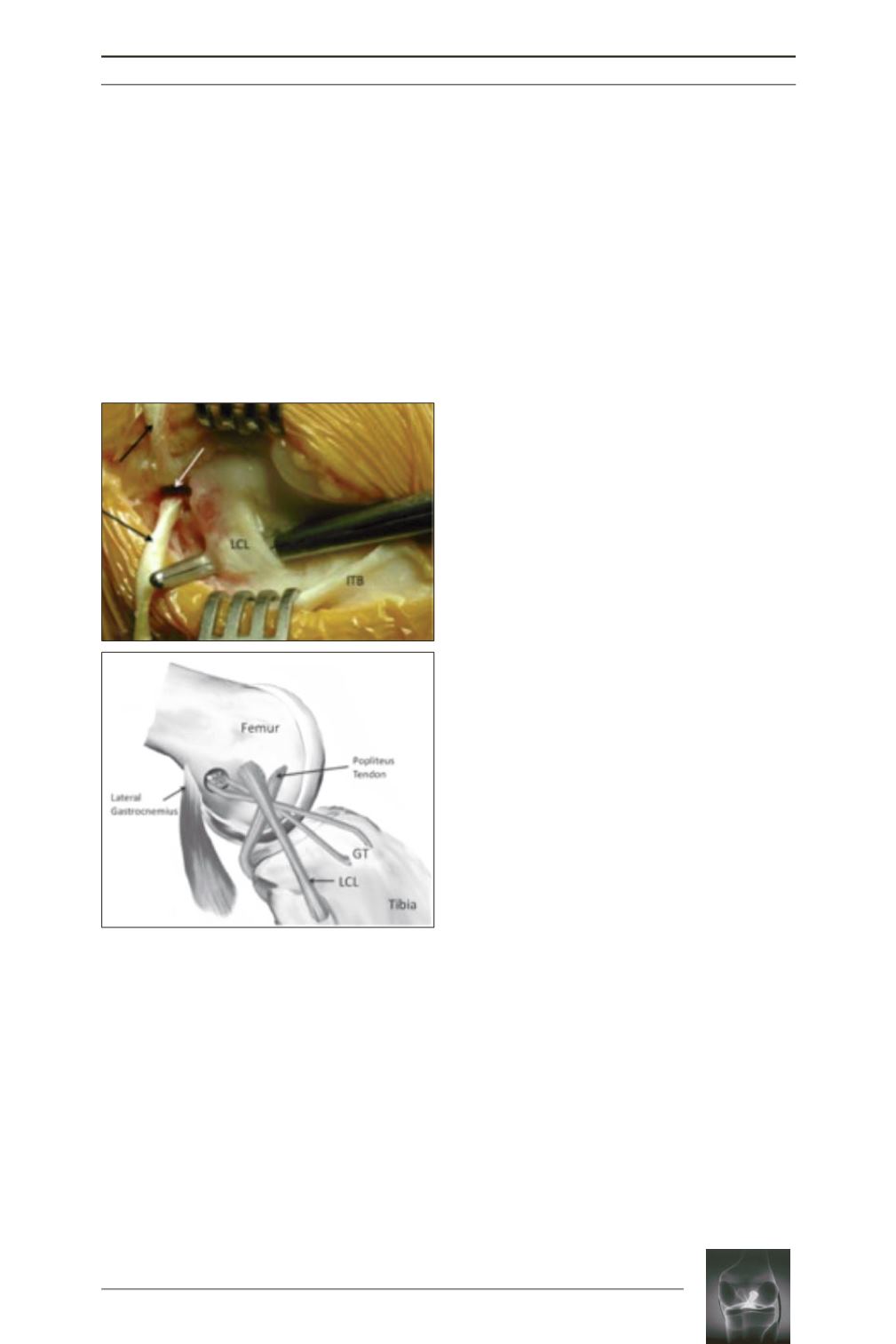
Fig. 6:
Per operative view (a) and line drawing (b) of
a right knee showing the KJT procedure, described
by Neyret.
From Magnussen and al. [23]
.
LCL, lateral
collateral ligament; ITB, iliotibial band; GT, Gerdy’s tubercle;
white arrow: tibial bone block; black arrows, two limbs of
gracilis tendon.
a
b