










 23 / 244
23 / 244

C. LUTZ, B. SONNERY-COTTET, M. DAGGETT, P. IMBERT
22
iliotibial tract layer (Kaplan’s fibers) attached
to the lateral intermuscular septum.
Once the ITB is reflected, an internal rotational
force is applied between 30 and 60° of flexion
of the knee to tighten the ALL as well as the
antero-lateral capsule (fig. 2a). This internal
rotation is absolutely essential to identify the
ALL: in neutral rotation, its relief can disappear
within the capsular thickness (fig. 2b). Once
this area is exposed, isolation of the lateral
collateral ligament (LCL) and the popliteus
tendon is carried out. The LCL is isolated by
applying varus stress and then dissected from
its distal insertion onto the head of the fibula to
its femoral insertion onto the lateral femoral
epicondyle (fig. 3). Care is taken to not incise
fibers overlapping the ALL.
Evaluation of the ALL physical characteristics
is then possible: the origin is determined by
placing tension on its proximal fibers; if
visualization of this origin is difficult because
of a confusion between proximal fibers from
the ALL and the LCL, these 2 structures can be
cut midbody and separated to see where the
main body of each structures is attached to the
lateral epicondyle, as recommended by
S. Caterine [1]. Identification of the tibial
insertion is done by placing tension on its distal
fibers. Measurement of length, width and
thickness complete this anatomical evaluation.
During the dissection, connections with
surrounding structures are also analyzed: ITB,
lateral meniscus, antero-lateral capsule.
ANATOMICAL
CHARACTERISTICS
(Table 1)
Femoral origin
One of the main conflicting points about the
anatomy of the ALL concerns its femoral
insertion. Most of the authors agreed on the
problems inherent to individualizing this
insertion because of the many connections with
the femoral insertion of the LCL and the fibers
coming from the fascia of the lateral vastus
muscle. The femoral attachment was initially
described by Vincent [12], Claes [2], and
Helito [5] to be anterior and distal to the
femoral LCL attachment, while Dodds [4],
Rezansoff [9] and our study [7] described
posterior and proximal attachments. Caterine
[1] explained these disparities by the existence
of anatomical variations and proposed a three-
stage classification according to the differences
in femoral and tibial insertions.
Fig. 2a:
ALL tight in internal rotation (blue pin =
Gerdy’s tubercle; yellow pin = femoral lateral
epicondyle, green pin = fibular head, dotted lines =
anterior and posterior ALL limits).
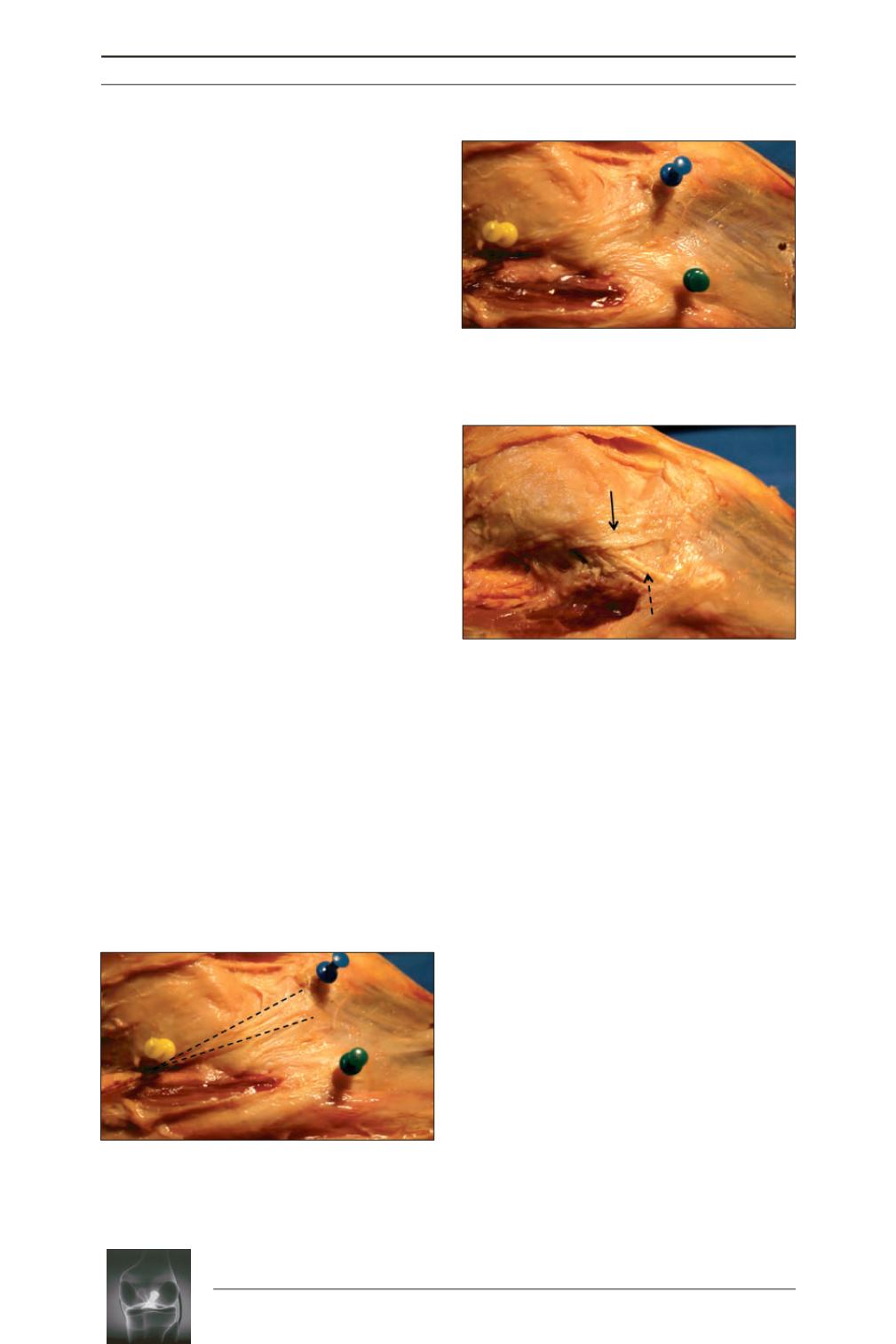
Fig. 2b:
Difficulties to located ALL in neutral rotation
(blue pin = Gerdy’s tubercle; yellow pin = femoral
lateral epicondyle, green pin = fibular head).
Fig. 3:
ALL (arrow) exposure after LCL (dotted
arrow) dissection and antero-lateral capsule
removing.
a
b