










 176 / 244
176 / 244

WHAT ARE THE INTRINSIC FACTORS IN ACL FAILURE?
175
Song
& al.
[15] conclude that the combination
of anterolateral plasty and ACL reconstruction
is effective in eliminating the PS phenomenon.
We propose that the association of SSD >9 mm
(Telos
TM
) with PS test 2+ or 3+ may require an
additional anterolateral plasty (modified
Lemaire). In a biomechanical study, Kittl
& al.
[16] demonstrate the surgical rationale of this
technique showing that a graft fixed proximally
to the lateral femoral epicondyle and running
under the lateral collateral ligament provides
the desirable graft behavior, without excessive
slackening or tightening of the plasty during
knee motion.
Deflexion osteotomy has to be considered
especially after the failure of two or more
consecutive ACL procedures, when PTS is
higher than 12° and in case of meniscal lesions
or previous meniscectomy, which could
exacerbate the effects of a high PTS [8] (fig. 5).
Dejour
& al.
[8] report a mean PTS reduction
from 13,2°±2,6° pre-operatively to 4,4°±2,4°
post-operatively and a mean SSD decrease
from
11,7±5,2mm
pre-operatively
to
4,3±2,5mm post-operatively. However, the
authors conclude that the correction of
excessive PTS should be considered also in the
first revision ACL reconstruction as this can
reduce the risks of failure.
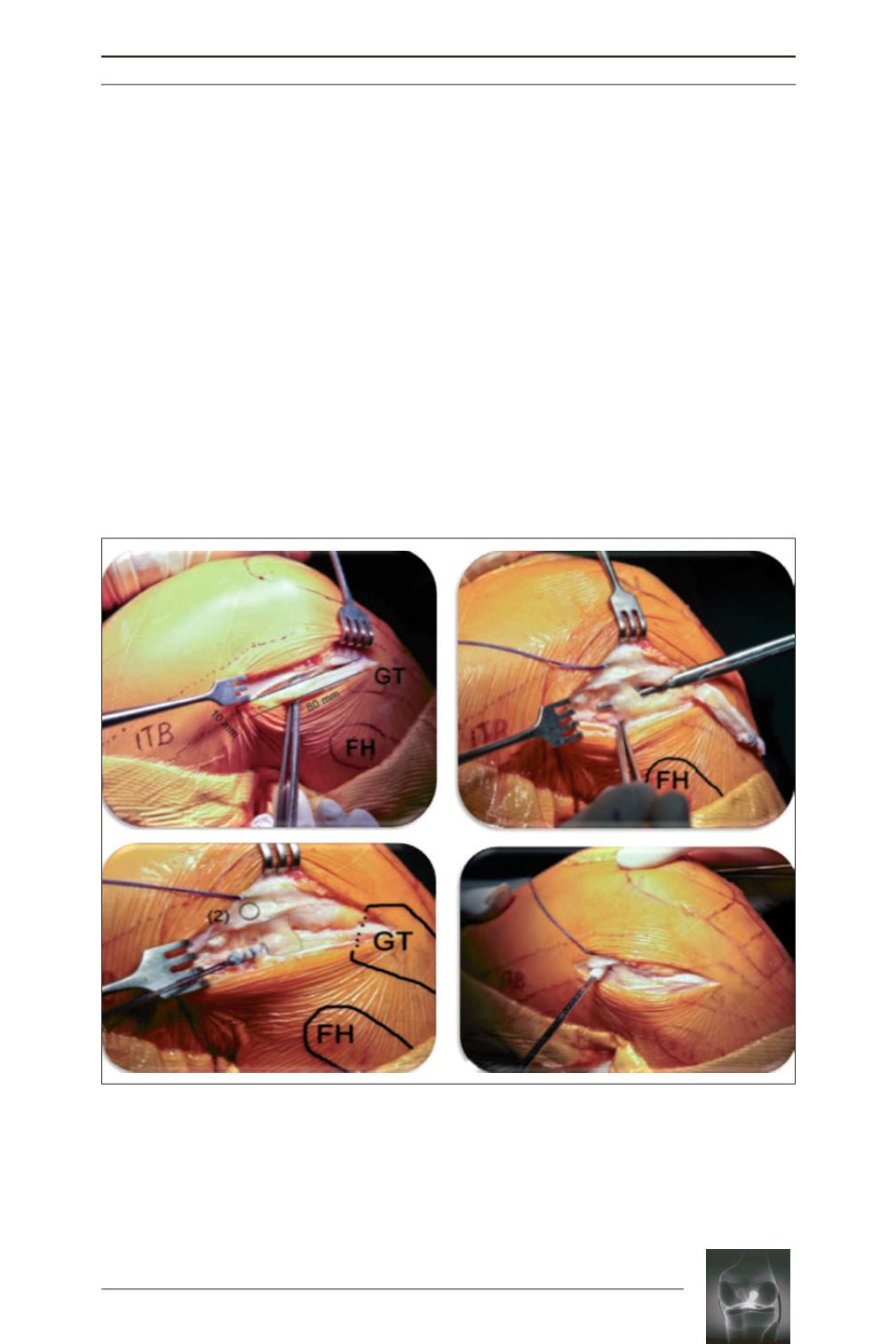
Fig. 4:
In case of pivot shift 2+/3+ and SSD > 9 mm (Telos
TM
), an anterolateral plasty (modified Lemaire) can
be associated to the ACL reconstruction. (a) A strip of Ileotibial band (ITB) is harvested keeping intact its
distal insertion. (b) The lateral collateral ligament (LCL) is identified and two mini-arthrotomies (posterior
and anterior to LCL) are performed. (c) The strip of ITB is pulled under the LCL. (d) An half tunnel is drilled
proximally to the lateral femoral epicondyle and the fixation is achieved with an interference bioabsorbable
screw.
a
c
b
d