










 77 / 244
77 / 244

J. CHAPPUIS, J. BARTH, J.C. PANISSET
76
During the first 6 to 12 weeks after surgery,
when conversion from mechanical to biologic
fixation is occuring, the fixation must be able to
withstand the demands of an accelerated
rehabilitation program.
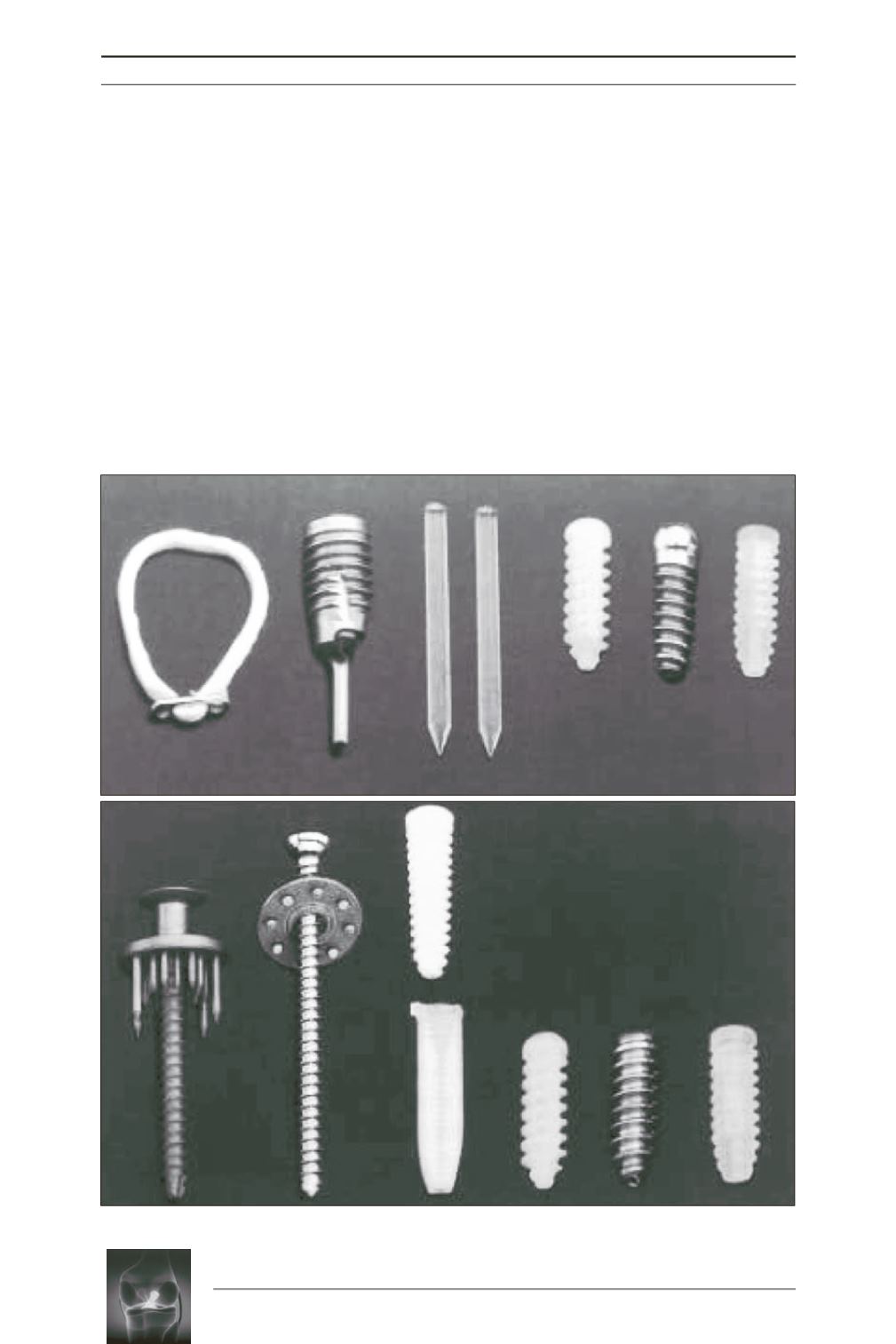
There are a variety of methods by which the
bone and soft tissue grafts can be fixed, and this
can be done either in the bone tunnel or through
a cortical based fixation away from the joint [3]
(fig. 1). Historically, the revolution was the
Kurosaka screw [4] (fig. 2).
Fixation strength is especially important on the
tibial side, which is usually the site of fixation
failure, because the metaphyseal region of the
tibia has less bone density than the femur and
the graft experiences forces that are more
collinear within the tibial tunnel [5].
Efficiency of graft fixation depends on the
characteristics of the fixation devices, on the
site of fixation (aperture or nonaperture), on the
density of the bone (tibia or femur) and on the
type of graft.
Fig. 1:
From Kousa and coworkers
[3]