









 121 / 280
121 / 280

On the radiological
Δ
ATT, a displacement
difference of 1 to 3 millimeters is considered
to be suggestive for a partial ACL insuffi-
ciency. Nevertheless, we don’t have any infor-
mation on the actual anatomical amount of
ACL elongation.
A cadaveric study showed an anterior tibial
translation of 0.6 mm [18] after section of
the posterolateral bundle and approximately
0.9 mm [1] to 1.3 mm [21] after section of
the anteromedial bundle.
But these cadaveric studies do not reproduce
the true clinical situation because they do
not evaluate the importance of ACL lengthe-
ning [1, 18, 21] and the plastic deformation
in the remaining fibers.
During arthroscopy, the diagnosis is often
difficult. Even after removal of subsynovial
bleeding, two different macroscopic aspects
of the ACL can be observed: a discontinuity
of the fibers or a continuity (i.e. no rupture).
In 1973, Noyes [24] elegantly described the
diagnostic problem: “The visual determina-
tion of continuity of a ligament at the time of
operative exploration is often the determi-
ning factor in terms of treatment, but it may
give an inadequate determination of the
extent of ligament disruption, residual elon-
gation, or damage to the blood supply which
has actually occurred”.
In summary, clinical examination and MRI
allow us to diagnose a partial tear. We know
the possible consequences of the tear and the
subsequent laxity on the arthrometer. But we
don’t know the anatomical partial tear cor-
responding to the laxity. And as said Lintner
[21] : “if a significant laxity is present this
actually represents anatomic rupture of one
bundle with interstitial lengthening of the
remainder of the ligament, resulting in a
functionally complete tear of the ACL”.
WHICH ARE THE
ASSOCIATED LESIONS WITH
A PARTIAL ACL TEAR?
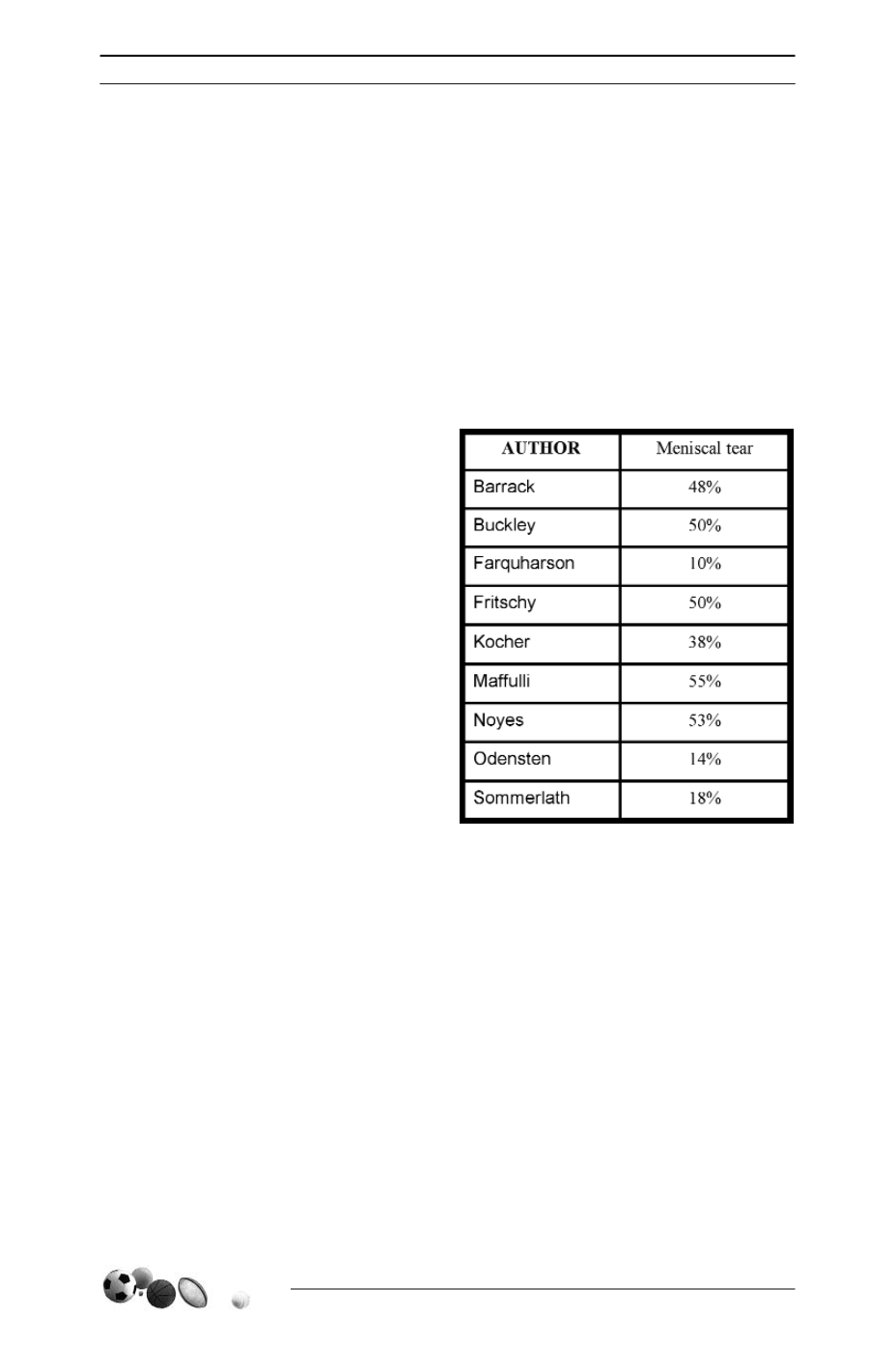
Approximately fifty per cent of meniscal tears
(10%-55%) [Table 1] and twelve per cent of
bone contusions (predominantly in the late-
ral compartment (90%)) [34] are associated
with a partial ACL tear. The rate of an asso-
ciated MCL tear is difficult to determine.
WHAT IS THE NATURAL
EVOLUTION OF PARTIAL
ACL TEAR?
The risk of a partial tear evolving to a com-
plete tear is known. The size of the partial
tear is considered a risk factor for a comple-
te rupture by some authors. Noyes [25]
found that when over fifty per cent of the
13
es
JOURNÉES LYONNAISES DE CHIRURGIE DU GENOU
120
Table 1