










 13 / 324
13 / 324

METHODS
Since 1988, we have performed stress X-rays
in order to plan the release procedure during
TKA and to analyze the reducibility of the
varus or valgus deformity. Between March
1988 and August 2007, one thousand nine hun-
dred-fourteen TKAs were carried out in our
department. All data have been collected into a
database for further studies. This study only
included the patients with medial tibiofemoral
osteoarthritis. Exclusion criteria were as fol-
lows: lateral compartment osteoarthritis, infla-
matory arthritis, villonodular synovitis, neuro-
pathic arthropathy, previous high tibial osteo-
tomy, previous ligament injury and fracture
around the knee joint. One hundred and twen-
ty patients’ files were randomly selected from
this database with regard to the study criteria
without the knowledge of soft tissue release
procedures. There were 84 females and
36 males. The average age of the patients at
the time of the operation was 71.3 ± 7.1 years
(range, 56 to 92). There were 65 right and
55 left knees. To accomplish the purpose of the
study knees were divided into three groups
according to the operative medial soft tissue
release reports during TKA surgery, which are
described below:
• Group 1 consisted of 64 knees:
Capsule and
deep MCL.
• Group 2 consisted of 37 knees:
Capsule and
deep MCL + Pie crust superficial MCL at
the joint line.
• Group 3 consisted of 19 knees:
Capsule and
deep MCL + Superficial MCL distal on the
tibia to the pes anserinus insertion.
Radiographic measurements
Standard preoperative evaluation of the align-
ment and bone/soft tissue structures included
weight-bearing bipodal long-leg radiographs,
anteroposterior/lateral monopodal stance radio-
graphs, schuss view, skyline view and varus-
valgus stress radiographs of the affected knee.
• Hip-knee-ankle mechanical angle (HKA=
intersection of the lines joining the center of
the knee to the center of the femoral head and
the center of the ankle, respectively) was
measured under a full-limb weightbearing X-
ray to clarify the relation between the align-
ment [9] and the knee joint laxity. The varus
malalignment was defined as the hip-knee-
ankle mechanical angle inferior to 180°.
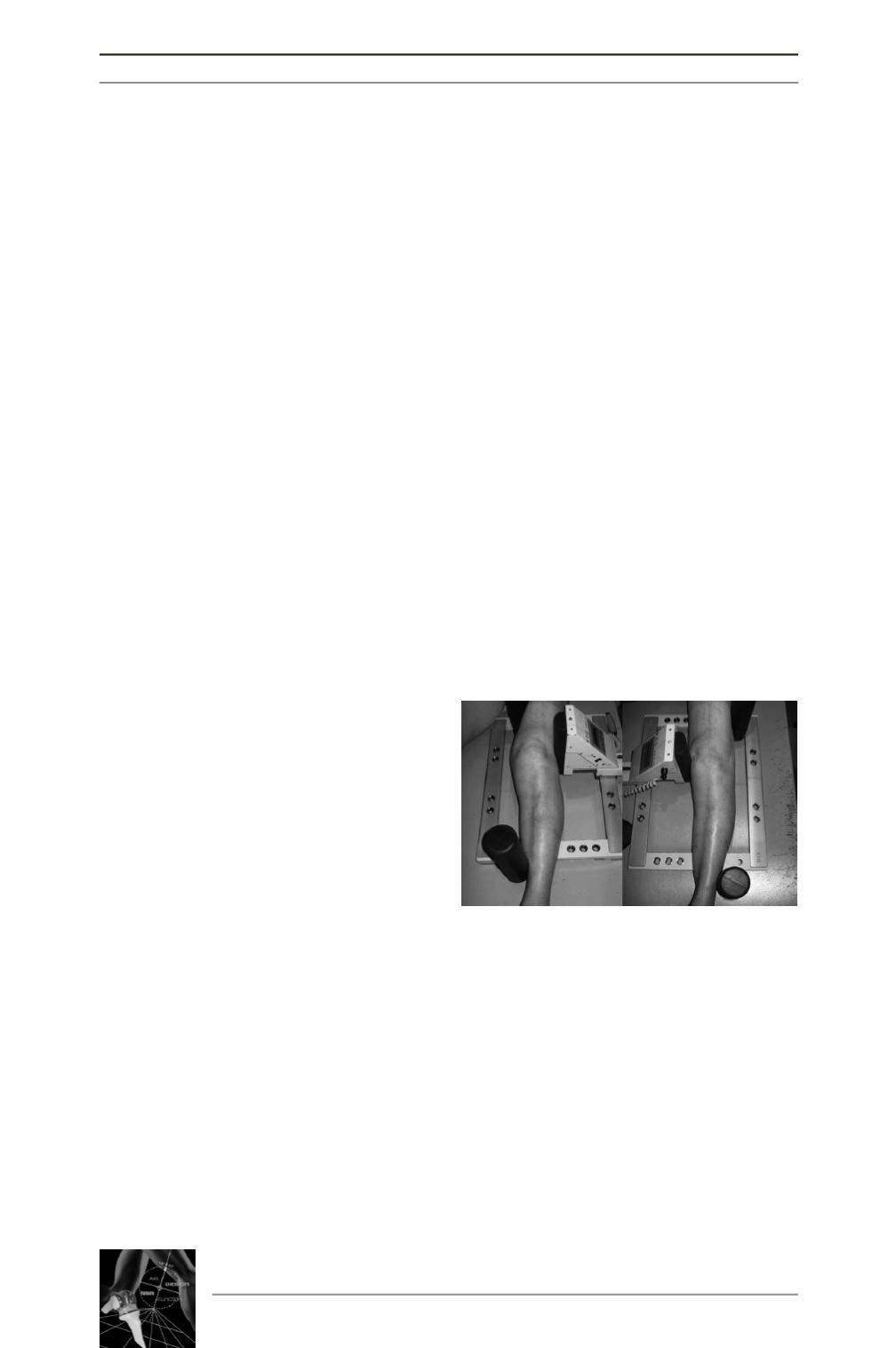
• The stress radiographs were performed on
the patient lying supine using a standardized
technique with KSG-EMO 30 arthrometer
(Lehmann Medizintechnik, Mainburg,
Germany). For the valgus/varus stress test,
130 N was applied across the knee either
medial or lateral joint line (fig. 1) in 0°-20°
flexion position. A tube was centered at the
knee joint line at a distance of 1 meter from
the cassette with patella looking forward.
Measurements were performed on the
varus/valgus stress radiographs using three
different methods:
- The femorotibial anatomical angle (FTA),
- The femorotibial separation angle (FTS),
- And the medial and lateral compartment
joint space widths’.
The femorotibial anatomical angle (FTA)
was defined as the intersection of two lines.
The first line was drawn from the midpoint
of the tibial spines to a point that was bisec-
14
es
JOURNÉES LYONNAISES DE CHIRURGIE DU GENOU
12
Fig. 1 : Preparation of the knee for the
varus/valgus stress radiologic examination.
The knee was fully extended as the pain allo-
wed the patient, and placed in the KSG-EMO
30 arthrometer. For the varus/valgus stress,
a consistent 13dN force is applied either
medial or lateral aspect of the joint. And
positioning is checked with image intensi-
fier to avoid rotational errors.