










 156 / 324
156 / 324

Patients with smaller knees (predominantly
female) demonstrated large variability bet-
ween narrow and wide mediolateral dimen-
sions, irrespective of gender. The same was
true for larger knees (predominantly male).
This variability within gender could partially
be explained by morphotypic variation.
Patients with short and wide morphotype
(endomorph) had, irrespective of gender,
wider knees, while patients with long and nar-
row morphotype (ectomorphism) had more
narrow knees (p<0.01).
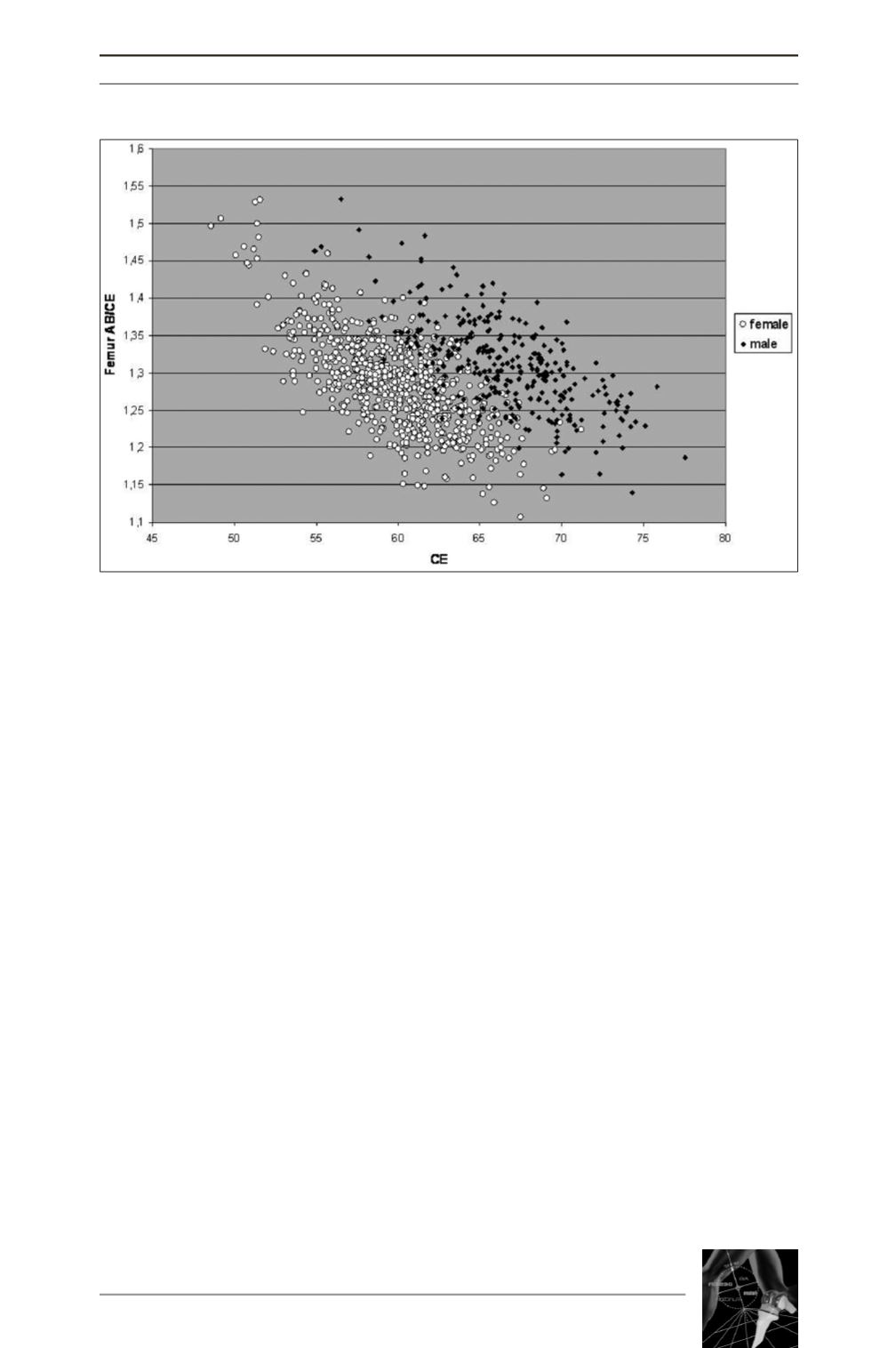
Both gender and morphotype were significant
predictors of the femoral aspect ratio (AB/CE)
(p<0.01).
Gender was the strongest predictor with
R²=0.48, indicating that 48% of the variability
in AB/CE was explained by gender, versus
R²=0.17 for morphotype, indicating that 17%
of the variability in AB/CE was explained by
the patient’s morphotype.
Tibial geometry
Of the 250 smallest tibia’s, 249 (99.6%) were
female, whereas of the 250 largest tibia’s 236
(94%) were male. Of the 500 patients with
intermediate size knees, 77 (15%) were male
and 423 (85%) were female.
No significant differences in mediolateral ver-
sus anteroposterior ratio’s were noted between
small, intermediate, or large tibia’s (fig. 4).
Female tibia’s were significantly smaller and
had greater mediolateral versus anteroposte-
rior ratio’s compared to male tibia’s. Patients
with short and wide morphotype (endomorph)
had, irrespective of gender, wider tibia’s, while
patients with long and narrow morphotype
(ectomorph) had more narrow tibia’s (p<0.01).
Both gender and morphotype were significant
but weak predictors of the tibial aspect ratio
(AB/CE) (p<0.01). Morphotype was the stron-
gest predictor with R²=0.04, indicating that
4% of the variability in AB/CE was explained
THE INFLUENCE OF MORPHOTYPE AND GENDER ON THE SHAPE OF THE KNEE IN TKA PATIENTS
155
Fig. 3 : Graphical demonstration of the femoral aspect ratio
in function of the femoral size (CE) and gender of the patient.