










 157 / 324
157 / 324

by morphotype, versus R²=0.02 for gender,
indicating that 2% of the variability in AB/CE
was explained by the patient’s gender.
DISCUSSION
Today there is growing evidence that male and
female knees are different in geometry [7, 8,
16, 19, 20, 21]. For this reason, it seems logi-
cal to consider the development and use of
gender specific knee implants that more close-
ly replicate the gender specific anatomy, there-
by optimizing the implant fit to the patient’s
individual geometry [1, 4, 5, 9, 10, 11].
The problem is however that even within gen-
der there seems to be a high variability in distal
femoral and proximal tibial dimensions
amongst patients, which suggests that other
factors than gender seem to have an influence
as well [17]. Also, it is well known that patients
undergoing TKA are predominantly female,
and therefore the need for gender specific
implants may be further questioned [9, 13].
In this work we have tried to provide a better
insight into this matter, by investigating the
distal femoral and proximal tibial geometry in
1000 consecutive TKA patients that were ope-
rated in our centre.
Our study demonstrates that when looking at a
consecutive group of patients undergoing
TKA, the small sized knees are almost always
female knees, whereas the larger sized knees
are almost always male. 98% of the 250 smal-
lest sized femurs and 99.6% of the 250 smal-
lest sized tibia’s in our study were female,
which suggests that it makes little or no sense
to provide separate male implants for the 25%
smallest sizes. Likewise for large sized knees,
which were predominantly male. 94% of the
250 largest sized tibia’s and 81% of the 250
largest femurs of our study were male, which
suggests that for the larger sizes a single, male
implant geometry should be sufficient.
The situation was somewhat different in the
group with intermediate size knees, where
both a fair number of male and female patients
were present.
Our study has demonstrated that female knees
had on average more narrow distal femurs
compared to male knees. Each mediolateral
over anteroposterior femoral ratio that we stu-
died was indeed significantly smaller for
female patients compared to male, and there-
fore confirms what other authors have publi-
shed before [8, 16, 19, 20]. At first sight, this
may seem paradoxical since our study has also
demonstrated that small knees are significant-
ly wider in mediolateral versus anteroposterior
14
es
JOURNÉES LYONNAISES DE CHIRURGIE DU GENOU
156
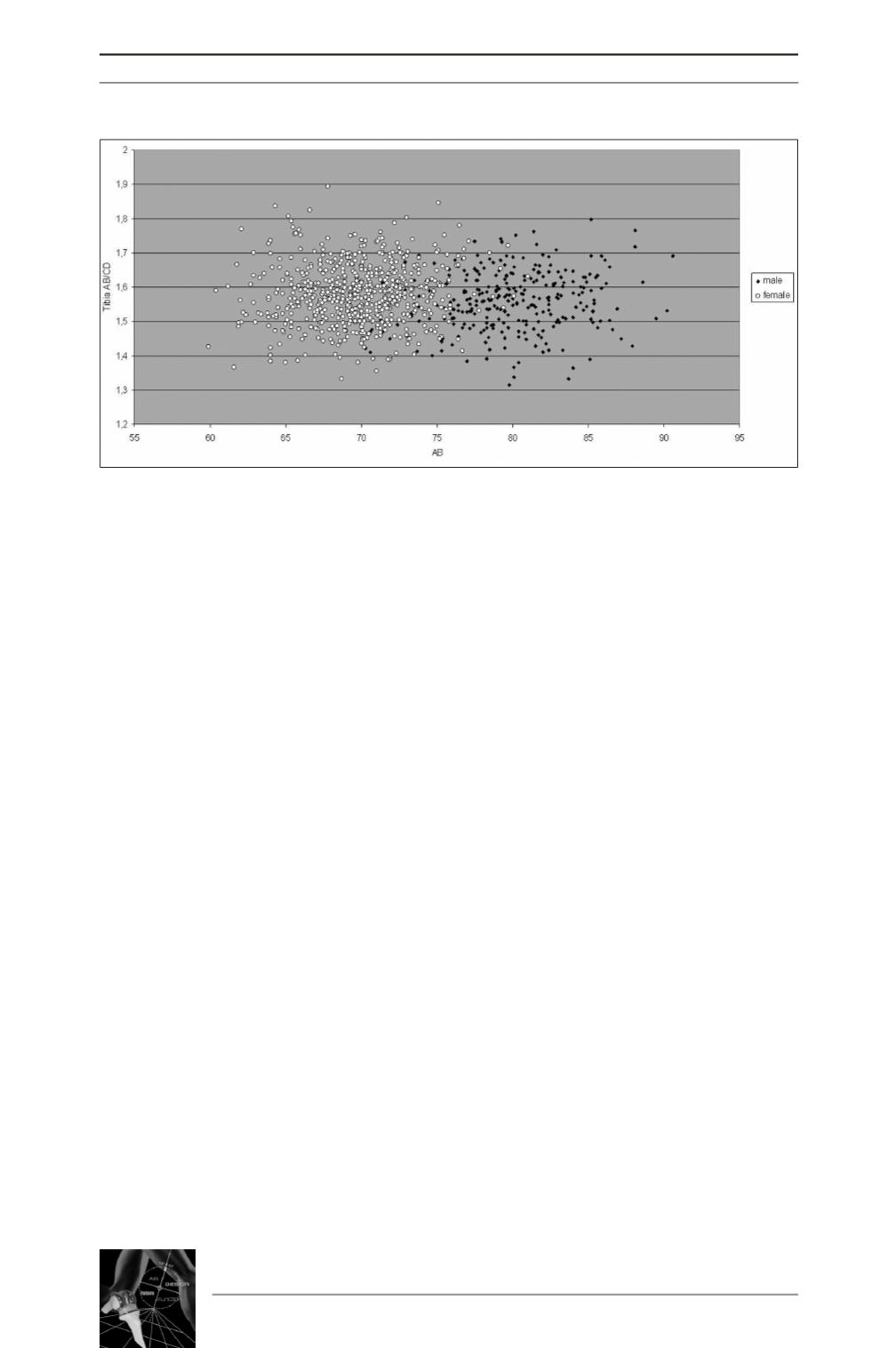
Fig. 4 : Graphical demonstration of the tibial aspect ratio
in function of the tibial size (AB) and gender of the patient.