










 222 / 324
222 / 324

possible because having made a small distal
femoral cut, a minor posterior resection is
enough to create the same flexion space.
In this way, we can distalize and however to
not rise the articular rim and re-establish the
posterior condylar offset: both critical factors
for biomechanical recovery and extensor appa-
ratus functioning.
Clinical experience with TKA has shown that
bone cut location and selection have relevant
effects on the final outcome.
A recent study, using two mathematical
models of the same knee prosthesis design,
showed the changes in knee forces along the
entire extensor apparatus (Adravanti P., sub-
mitted). The aim of the work was to use a com-
putational model of the Kansas Knee
Simulator (KKS) to investigate the effects of
the choice of femoral and tibial component on
several mechanical outputs that might be asso-
ciated with surgical outcome following total
knee replacement. Specifically, changes in
reaction forces and contact pressures between
the components, changes in extensor muscle
forces and changes in patello-femoral joint
kinematics during walking gait were investiga-
ted for a model knee reconstructed using two
different combinations of femoral and tibial
components from the same range of implants.
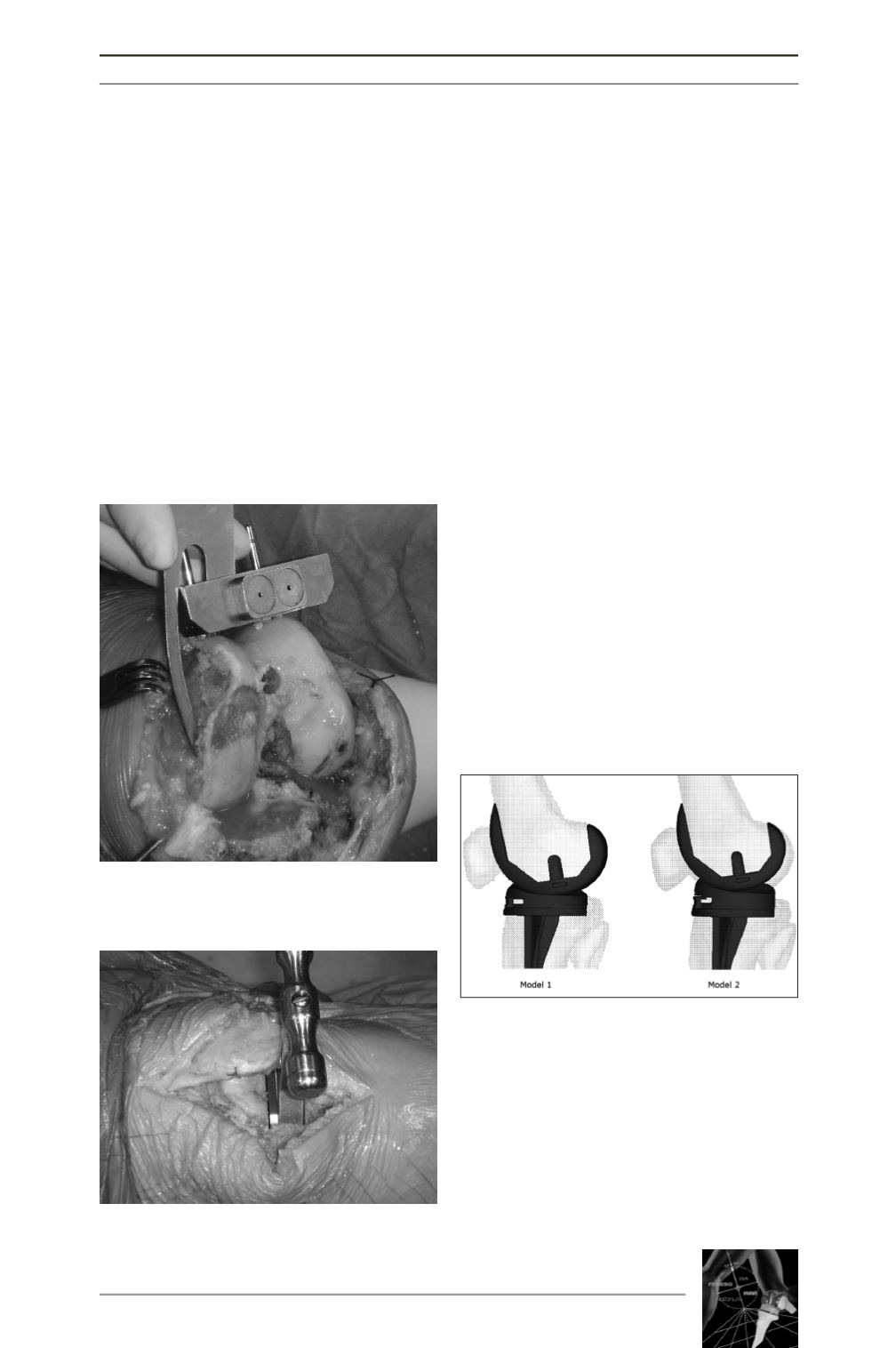
In the first model, the bone cuts were made to
re-establish the height of the articular line
using a total tibial thickness of 10mm above a
tibial resection cut of 10mm. In the second
model, the tibial resection was cut to 10mm
using a tibial thickness of 14mm. This means a
femoral resection, whether distal or posterior,
of more than 4mm and a small cut (4mm) can
be made to obtain the same flexion-extension
spaces in both models (fig. 3).
While the computational model predicted that
most kinematic and kinetic outputs, including
tibio-femoral and patello-femoral joint
motions, contact forces, pressures and areas
were similar for Model 1 and Model 2, there
was a dramatic difference in the extensor
BONE CUTS FROM THE JOINT-LINE
221
Fig. 1 : Limited femoral distal cut resection.
Fig. 2 : Knee balancing in extension
Fig. 3 : The two different models of the com-
putational study by the Kansas Knee
Simulator (KKS).