










 223 / 324
223 / 324

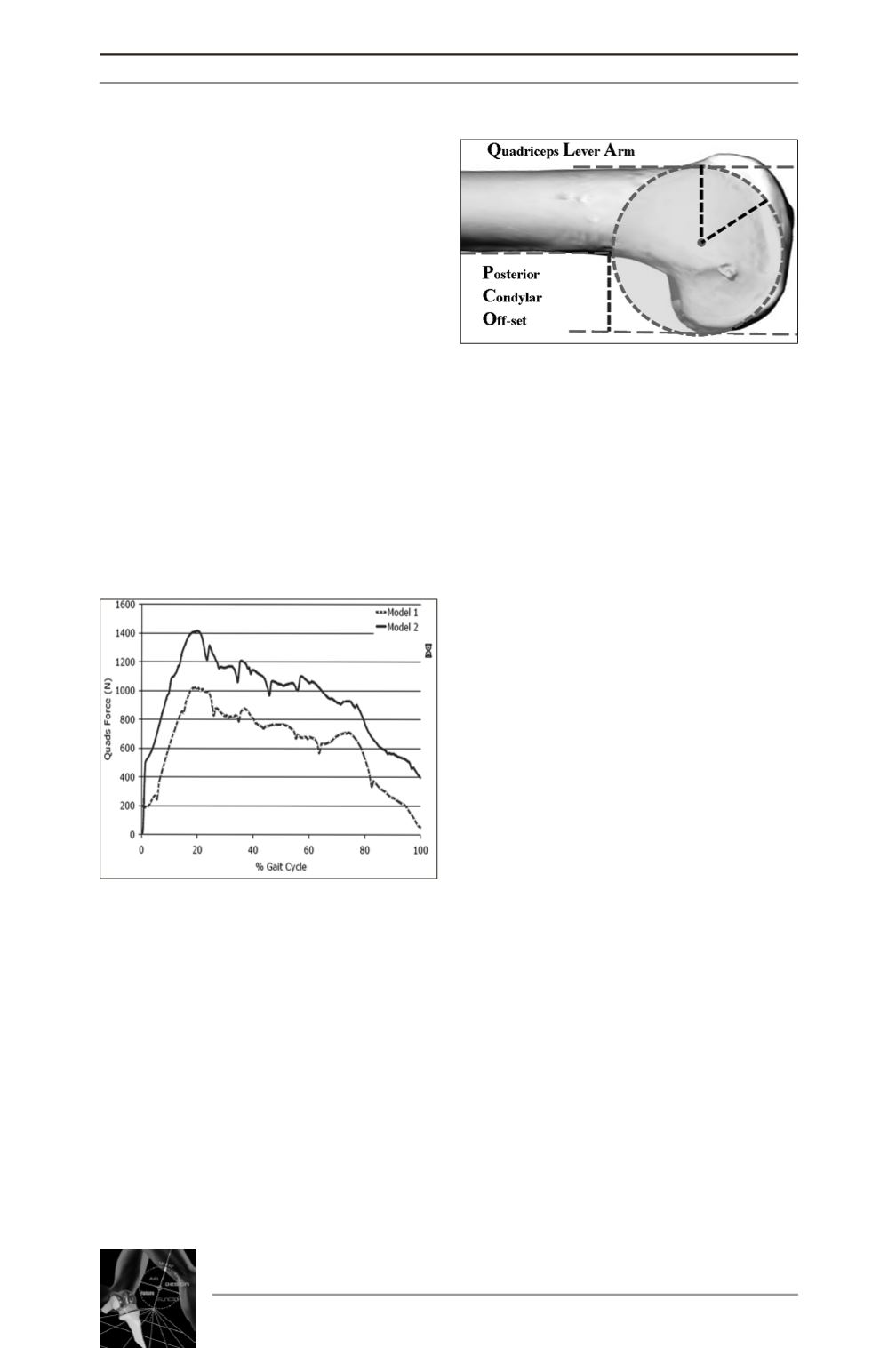
muscle forces necessary to flex and extend the
knee, these force being typically 40% higher
for Model 2 than for Model 1. For a patient to
reproduce the same knee motion with a knee
reconstructed as in Model 2, they would need
to generate approximately 40% greater exten-
sor muscle force throughout the gait cycle in
order to do so (fig. 4). Given such a large
increase in the extensor muscle force required,
what is more likely is that the knee motions
would be compromised and that a patient with
a knee reconstructed as in Model 2 would be
less likely to be able to reproduce normal knee
function and therefore more likely to report
poor outcome (Adravanti P
et al.
, submitted).
In order to correctly choose the resection
dimensions of the posterior cut and to obtain
correct femoral extrarotation, we believe in the
utility of spacers to measure the volume of
flexion space prior to perform the posterior cut.
A fundamental point is to reconstruct the AP
size of the distal femoral epiphysis in order to
re-establish quadriceps leverage and the poste-
rior condylar off-set (fig. 5); the latter one is
fundamental to restore the normal joint line
height in flexion. An undersized femoral com-
ponent anteroposteriorly compared to the natu-
ral femoral epiphysis reduces quadriceps leve-
rage and increases the force on the femoropa-
tellar surface, thus increasing the risk of ante-
rior knee pain and reducing joint function.
During normal activities of daily living such as
stair climbing, the load bearing force on the
articular surface can reach up to three times a
person’s body weight; during maximal flexion,
the force on the femoropatellar surface can
increase by up to seven to eight times body
weight, or nearly more than 150% the force on
the femorotibial surface.
Reconstruction of the posterior condylar offset
is essential for obtaining good range of motion
in flexion. This is possible only with modular
femoral components, i.e., components that dif-
fer minimally in size, which will then enable
us to posteriorize as far as possible the compo-
nent, while maintaining a correct anterior cut,
without notching or creating anterior overload,
and particularly without compromising flexion
and extension spaces [17, 18].
With prosthesis designs, with dimensional gap
of 3-4mm, the posterior offset can be recons-
tructed only by translating the component
anteroposteriorly, but they more often allow
for notching the anterior cortical surface or
stuffing the patellofemoral compartment ins-
tead [17, 18] which for each additional milli-
meter reduces flexion by 6 degrees [19].
By the same token, variation of only 1mm in
the posterior offset leads to a variation of
flexion of 6 degrees [18]. And because poste-
rior offset is also fundamental for good recove-
ry of flexion [20]. In total knee replacement
one should bear in mind that the knee is com-
posed of three compartments and that evalua-
tion of the patellofemoral compartment is key
14
es
JOURNÉES LYONNAISES DE CHIRURGIE DU GENOU
222
Fig. 4 : In model 2 patients would need to
generate approximately 40% greater exten-
sor muscle force throughout the gait cycle
respect to model 1 patients.
Fig. 5 : QLA (quadriceps lever arm)
and PCO (posterior condylar off-set).