










 254 / 324
254 / 324

DISCUSSION
Temporospatial data is an important factor to
assess knee function and kinematics.
Andriacchi showed that a painful knee results
in slower walking speed and reduced stride
length [12]. At the same time increased double
stance support time is common after TKA
which was found in both navigated and con-
ventional groups. However, a difference in
favour of the navigated group was found
between the two series which may suggest
subtle improvement in overall proprioception
or alignment so that navigated patients have
greater walking confidence than conventional.
Indeed meta-analysis reported improvement in
coronal and sagittal knee implant orientations
[18]. A recent x-rays alignment audit of 1000
postoperative TKA performed with conven-
tional versus navigation techniques demon-
strated again an improvement in overall align-
ment which could explain the results of our
study [19]. The low number of patients in this
study prevented us to assess alignment diffe-
rences which represents a limitation.
However, even a perfect aligned TKA still fea-
tures abnormal kinematics most of the time. In
a recent study, Komistek described abnormal
kinematics in a series of 236 TKAwith various
PS and CR models (similar to those used on
our patients) in which 53% had posterior
motion of the lateral condyle and 43% experi-
enced posterior motion of the medial condyle
[8]. Indeed knee kinematics have not be fully
restored using navigation despite being better
than conventional. In 2008, in a cadaver exper-
iment using fluoroscopy, Bull showed that
screw-home mechanism and posterior femur
translation were both lost in navigated knee
[20]. Knee kinematics depend of various fac-
tors and alignment is just one of them.
Nevertheless better leg alignment after TKA
has been recently identified to result in better
functional outcome using navigation or not
[15, 16]. This study did not identify any clini-
cal differences after 6 weeks as well as one
year. Are these subtle differences between
standard and navigated knees related to better
adduction and extension moment or/and
improvement ROM?
On the subject of the adduction moment first;
as mentioned already above Andriacchi
showed since 1997 that 70% of the leg load
goes through the medial compartment of the
knee joint. The load asymmetry results from
the adduction moment during gait cycle. Any
varus malalignment increases adduction
moment and medial loading. Coronal moment
analyzed in this study seems more reliable
than sagittal plane which should be cautiously
interpreted according to Hilding [11].
During stance, the location of the mass center
of the “passenger unit” (Head Arm and Trunk)
changes relative to the joints of the supporting
lower limb and this influences joint stability.
Bressler and Frankel noted a brief increase
(approximately 20%) in both the knee and hip
values at the beginning of loading response
during which supposedly the optimum stabili-
ty is essential [9]. Improving tridimentional
orientation of femoral and tibial implants as
ANALYSE À LA MARCHE DE DEUX SÉRIES HOMOGÈNES DE 40 PATIENTS OPÉRÉS DE PTG…
253
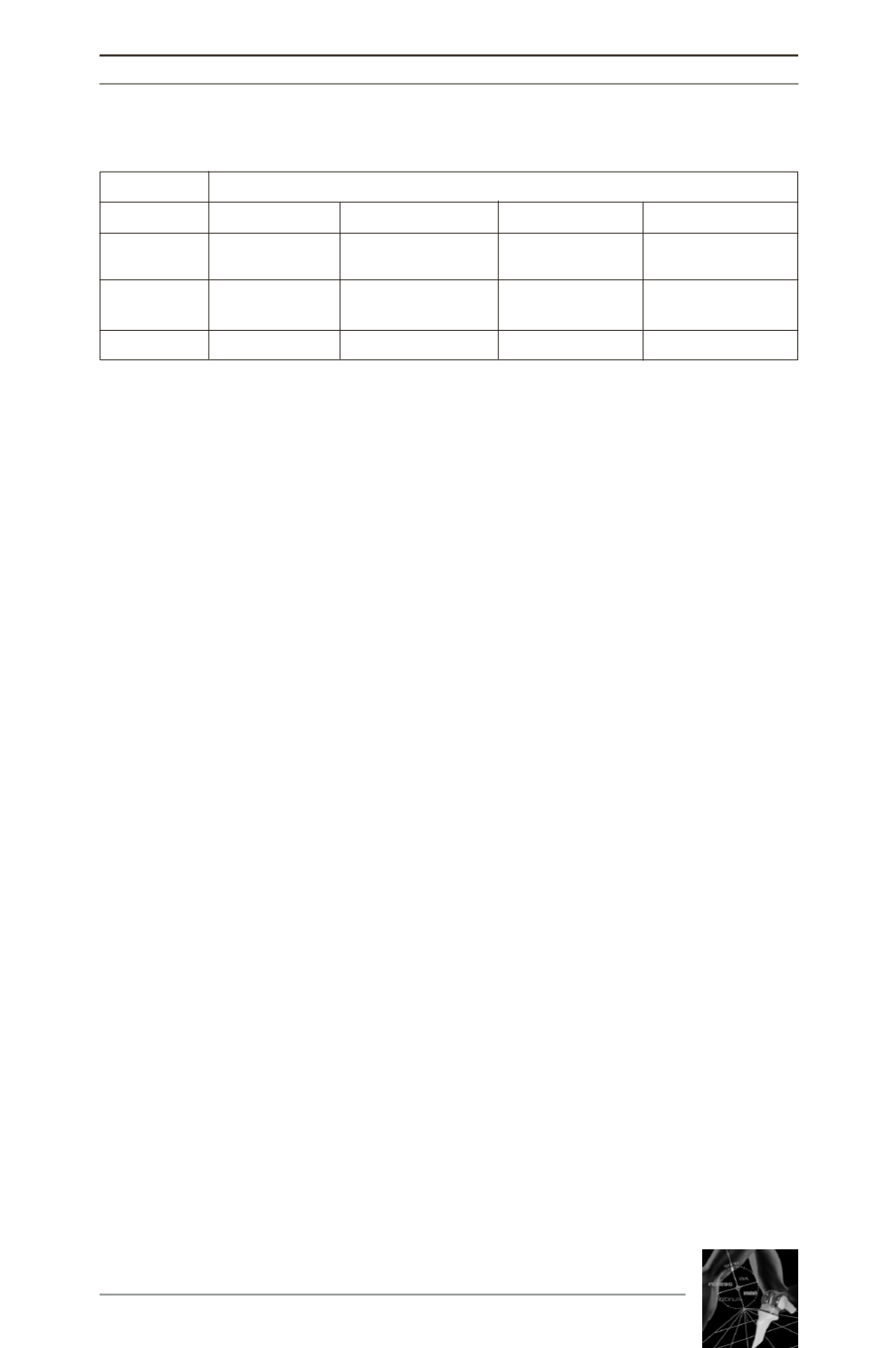
Subjects
Maximum knee flexion (degrees)
Level walking Chair rising/sitting Ascending stairs Descending stairs
standard
65.6 ± 22.5
82.5 ± 20.9
81.8 ± 28.3
86.1 ± 25.6
(p=0.009)
(p=0.01)
(p<0.0001)
(p<0.0001)
navigated
72.6 ± 17.5
92.8 ± 15.8
99 ± 8.6
106 ± 16.4
(p=0.74)
(p=0.64)
(p<0.0001)
(p<0.0001)
control
73.5 ± 17.9
93.5 ± 15.1
103.4 ± 14.6
119.5 ± 16.3
Table III: Gait analysis data
(p in standard = comparison to navigated and p in navigated = comparison to control)