










 188 / 460
188 / 460

187
Introduction
Since the documentation of trochlear dysplasia
as the most consistent anatomic factor present
in patients with recurrent patellar dislocation
[1], a number of surgical procedures for its
treatment has been introduced [2]. Trochleo
plasty procedures are designed to reshape the
abnormal trochlear groove and because they
involve a certain amount of technical difficulty
[3], they were initially accepted with skepticism
or reserved as salvage options [4]. But recent
literature contains several authors with
encouraging short and mid-term results on the
treatment of patients with patellar dislocation
and underlying high-grade trochlear dysplasia
leading to a great patellar instability and
patellar dislocations [5-13].
Trochlear dysplasia is a developmental
condition where the femoral trochlea loses its
normal concave shape to an abnormal flat or
even convex geometry [14]. Four basic
trochleoplasty procedures have been proposed.
Albee’s pioneer procedure involved the
elevation of the lateral facet in order to restore
normal anatomy [15]. The second procedure is
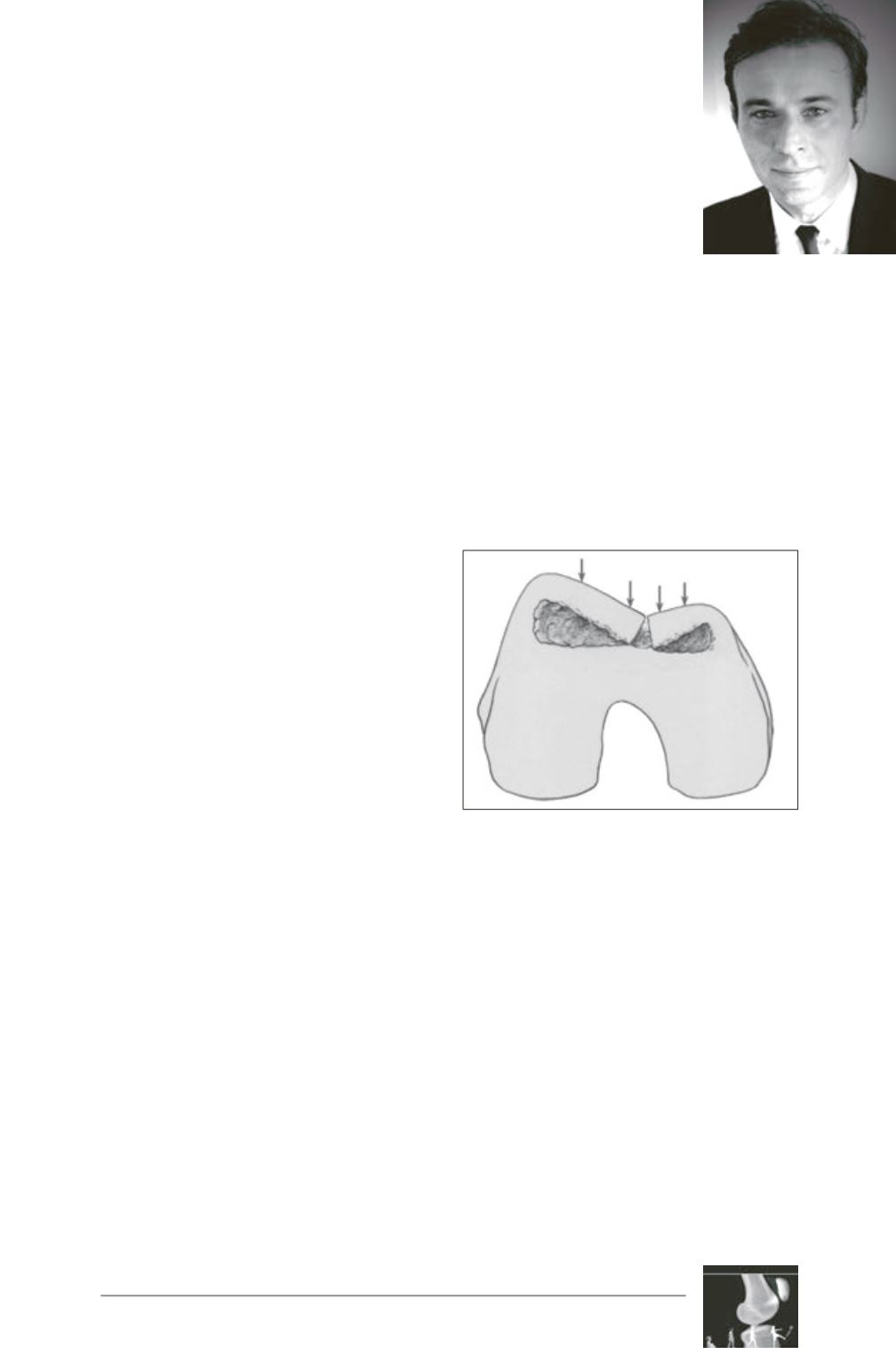
the “sulcus-deepening trochleoplasty”, which
was first proposed by Masse [16] and later
standardized by Henri [17] and David Dejour
[18] (fig. 1). The third procedure was introduced
by Bereiter and Gautier in 1994 [19], was later
followed by von Knoch [11] and is known as
the “Bereiter procedure”. An osteochondral
flake with only 2mm of subchondral bone is
elevated from the trochlea without osteotomy
of the condyle, and the distal femoral
subchondral bone is deepened and refashioned
with osteotomes and a high-speed burr. The
same procedure has been performed
arthroscopically by Blønd and Schöttle [13].
The fourth procedure is the “recession wedge
trochleoplasty” which was introduced by
Goutallier [20] in 2002 and has been embraced
by Beaufils [3]. In this technique, the shape of
the trochlea is not changed but the trochlear
bump is removed by a proximally-based wedge
and a subsequent pressure on the trochlea.
Sulcus deepening
trochleoplasty for the
treatment of recurrent
patellar dislocation with
underlying trochlear
dysplasia
P.G. Ntagiopoulos, P. Byn, D. Dejour
Fig. 1: The rationale of
the sulcus-deepening trochleoplasty.