










 284 / 460
284 / 460

The Treatment Evolution of Patellofemoral Degeneration, Arthritis, and Arthroplasty
283
Moving Forward - The Age of
Scientific Discovery (circa 1994 - the
Present)
In 1994, Brittenberg and Peterson fired the
biological restoration shot that was heard
around the world with their publication of the
autologous cartilage cell transplantion proce
dure [23]. However, despite early optimism
biological restoration of the patellofemoral
joint has proven challenging due to in large
part it’s inherently hostile biomechanical
environment (fig. D) (Table 1). A major step in
meeting the challenge of defining the operative
approach to symptomatic patellofemoral joint
occurred with the founding by Fulkerson and
Dupont in 1995 of the International Patello
femoral Study Group (IPSG). What has
followed has been a plethora of monographs
and papers addressing all aspects of anterior
knee pain and patellofemoral arthritis that
together have revolutionized thinking on the
subject (Table 2). After years of lateral side
strategy, a major focus during this era has been
the recognition of the importance of the medial
patellofemoral ligament in reducing extensor
instability [24]. It is a time for patella conserving
interventions such as partial lateral facetectomy
[25]. It is a time when the results of total knee
arthroplasty have drawn increasing scrutiny [2,
20]. There has been a renewed interest in
patellofemoral arthroplasty as a salvage
procedure to address advanced degeneration in
younger active patients who are unwilling to
accept the risks and potential revision of a total
joint (fig. E). This trend has set up a
philosophical divide between the traditional
“total joint surgeon” and the (for lack of a better
Table 2: Current Operative
Approaches for Patellofemoral Arthritis
Table 1: The Hostile Biomechanical
Nature of the Patellofemoral Joint
1. Arthroscopic debridement/
chondroplasty
2. Microfracture articular restoration
3. Lateral release
4. Soft tissue realignment of the extensor
mechanism
5. Osteotomies of the tibial tubercle
6. Mosaicplasty/autologous chondrocyte
implantation/biodegradable scaffold
7. Partial lateral facetectomy
8. Patellofemoral arthroplasty
9. Total knee arthroplasty
1. Intrinsically Lax
2. Incompletely Congruent
3. Dysplastic Prone
4. Overloaded/Overused
5. Highly dependent upon balancing
opposing extrinsically generated forces
that remain clinically unmeasurable
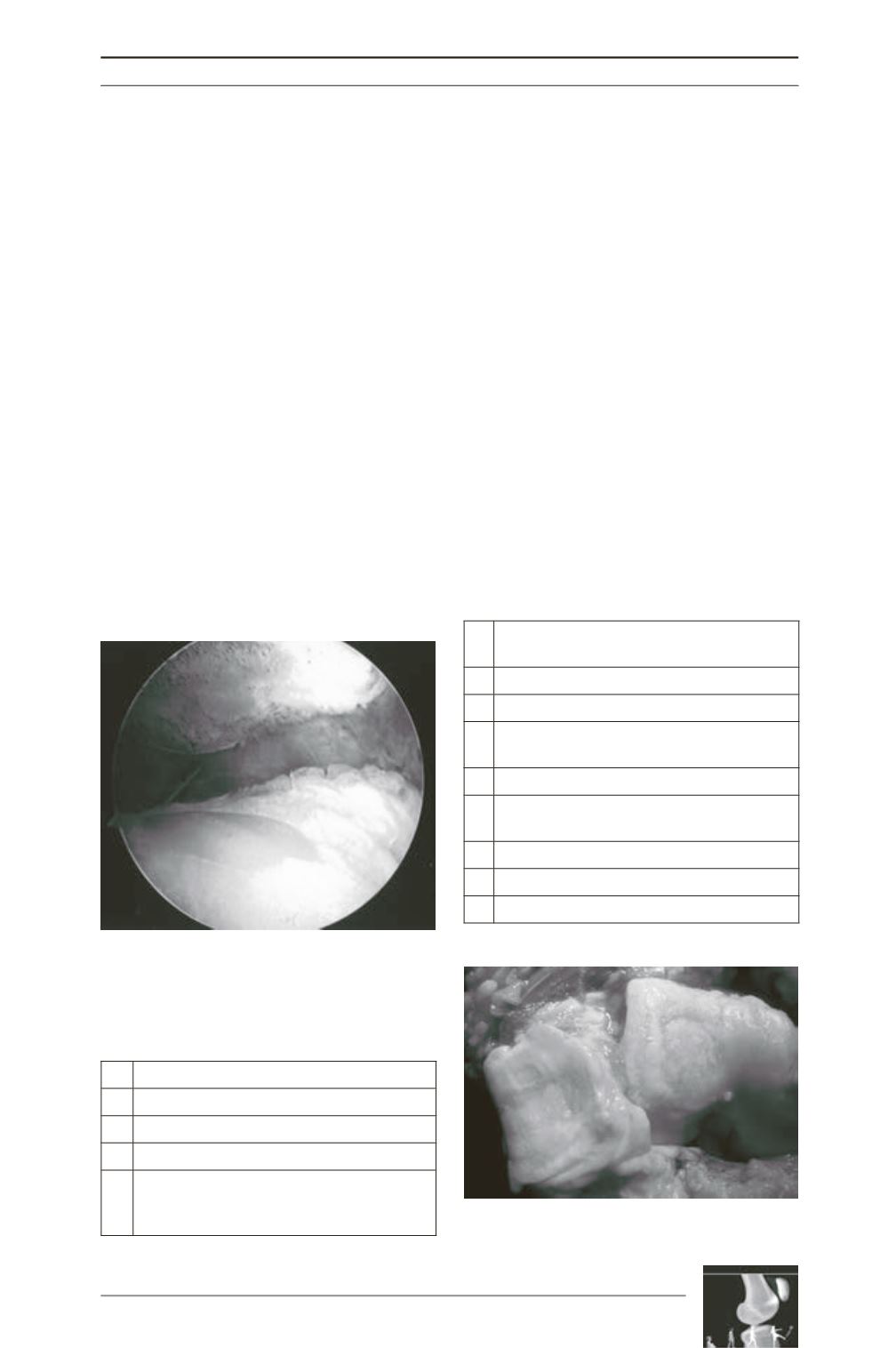
Fig. D: Arthroscopic view of advanced patello
femoral chondral degeneration. Note uncontained
bipolar lesions unfavorable to present restorative
procedures.
Fig. E: Patellofemoral arthritis
with trochlear dyplasia