










 325 / 460
325 / 460

P. Beaufils, M. Thaunat, D. Passeron, P. Boisrenoult, N Pujol
324
We hypothesized two causes:
- A lengthening effect of the lateral retinaculum
due to the lateral marginal patellectomy;
- Better positioning of the tibial implant in
external rotation. We know the key role of
optimal implants rotation in patellar tracking
[1, 6], specially in case of lateral patellar
subluxation. Lateral approach would allow a
better exposure of the tibial plateau while the
mediopatellar approach can induce internal
rotation tibial malposition because of
constraints imposed by the presence of the
patellar ligament.
In order to confirm this last hypothesis, we
conducted a computed tomography study,
measuring the rotation of the tibial implant
according to the type of approach [28].
In a prospective, comparative, non-randomized
study, CT scan was undertaken on 50 successive
knees in 50 patients at 3 months after primary
total knee arthroplasty, for gonarthrosis. Forty-
five knees were investigated. Fifteen knees
were operated by the lateral approach (8 with
osteotomy to elevate the ATT resting on its bed
without medialization and 7 without osteotomy
of the ATT) and 30 by the medial approach
(10 by the subvastus approach and 20 by the
medial parapatellar approach). The inclusion
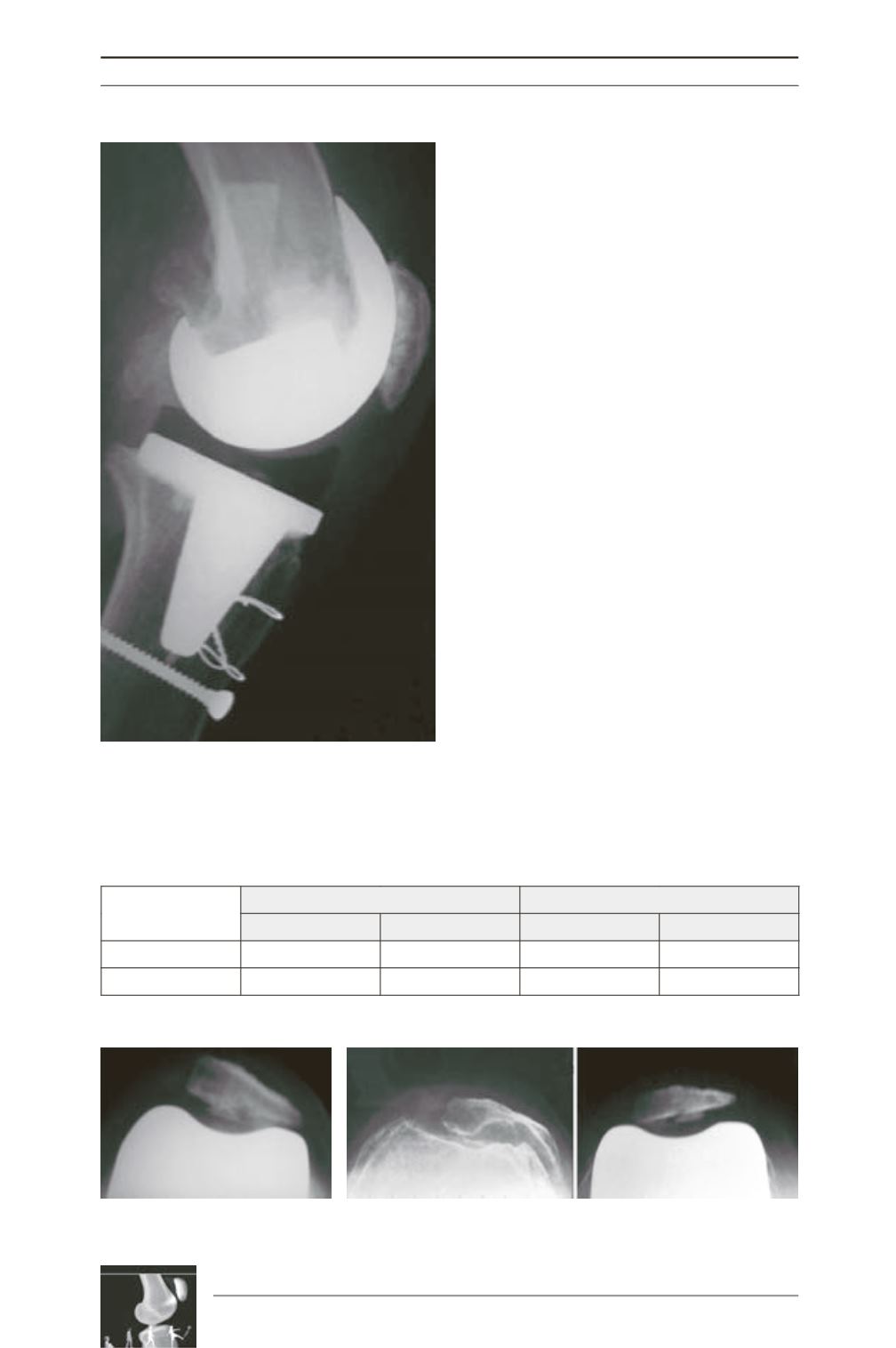
Fig. 2: Lateral approach with ATT elevation. Fixation
“in place” with two wires and one screw.
Fig. 3a: residual lateral tilt
with a medial approach.
Fig. 3b: residual medial tilt with a lateral approach
in a severely laterally subluxated patella.
Table 1 : Radiographic measurements in both groups.
Medial group
Lateral group
Preop
Postop
Preop
Postop
Gliding (mm)
7.6 ± 1.3
0.7 ± 1.8
9.7 ± 5.0
0.0 ± 0.0
Tilt (°)
+4.2 ± 3.6
-3.3 ± 5.4