








 149 / 242
149 / 242

Tibial slope and osteotomy: technicals aspects
149
Discussion
Nowadays, 2 main surgical techniques, cwhto
and owhto, are available and each has its
particular side effect. The choice of one or the
other depends on many criteria, and often on
the surgeon’s usual practices.
No study has assessed wedge positioning and
its impact on the tibial slope, except for Marti,
who put the wedge more posterior when he
associated osteotomy with anterior cruciate
ligament repair [10].
Moreover, it is difficult to compare results of
several studies, given the different methods to
measure tibial slope, especially when there is
no correlation between them.
Our study showed an increase in tibial slope of
about 0.4°. When we compared our results with
those in the literature, we found, on average, an
increase of about 3° [3-6, 10]. But in all of the
other studies, the positioning of the wedge was
never mentioned.
Joon [11] showed a difference in tibial slope,
depending on whether or not he cut through the
posterior cortex of the bone completely. For us,
the cortex must be cut through completely so as
to position the wedge as posteriorly as possible.
Noyes [12] showed that to have no modification
of the tibial slope after opening-wedge high
tibial osteotomy, a difference between anterior
and posterior gap is needed, with the posterior
gap twice as wide as the anterior gap, and for
each increase of one millimeter in the anterior
gap, 2 degrees of tibial slope is gained.
Posteriorpositioningofthewedgeautomatically
leads to a wider posterior gap.
Unfortunately, no study has yet compared
anterior positioning with posterior positioning
of the wedge and its impact on the tibial slope.
This issue has to be studied.
Conclusion
The cause of the increase in tibial slope after
OWHTO has not been totally elucidated, but
our study shows an encouraging way to go.
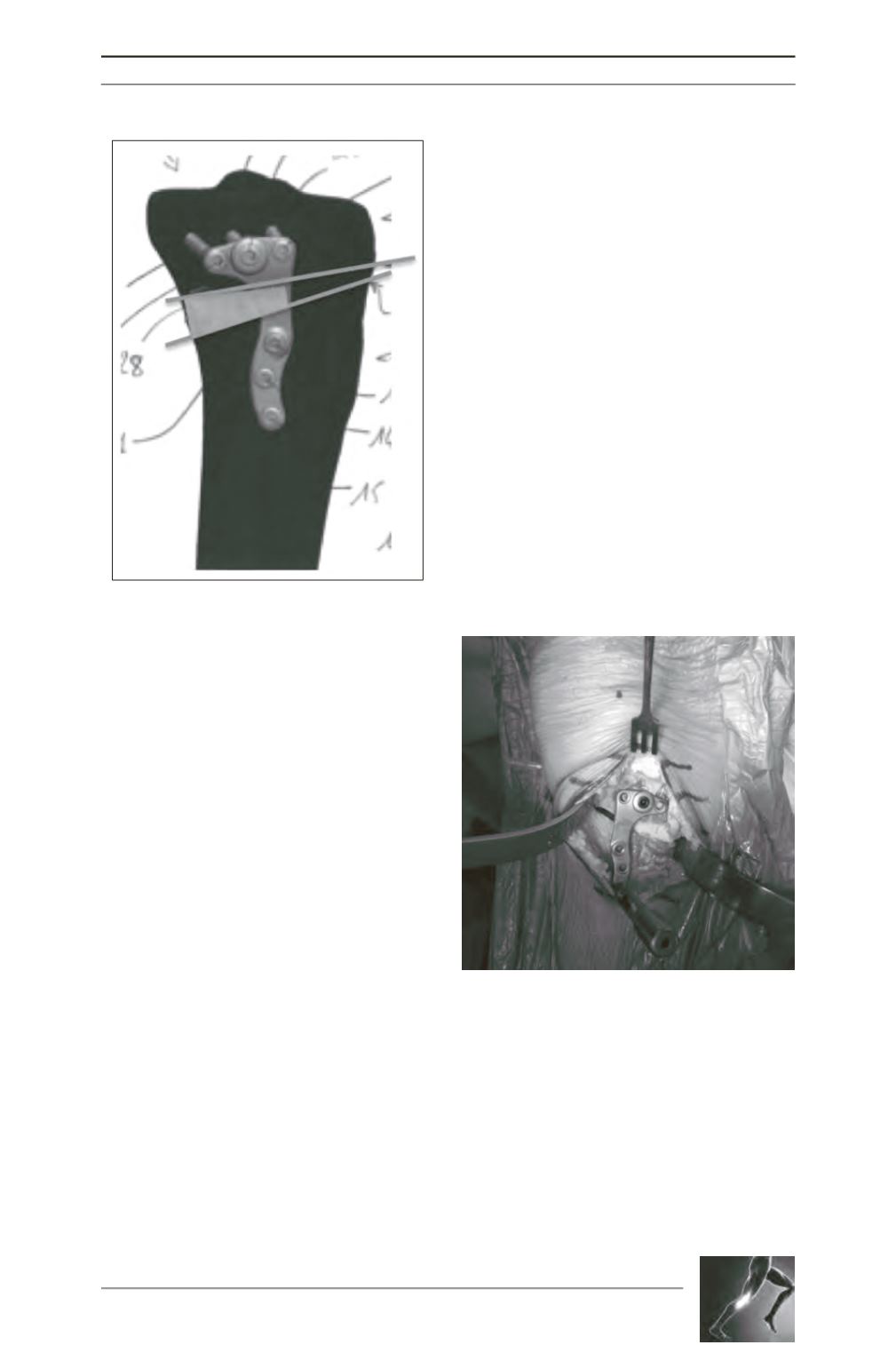
Fig. 3 : Example of posterior positioning of the
wedge.
Fig. 4: Profile view of the posterior positioning of
the wedge.