








 58 / 242
58 / 242

M. Saffarini, P.G. Ntagiopoulos, G. Demey, B. Le Negaret, D. Dejour
58
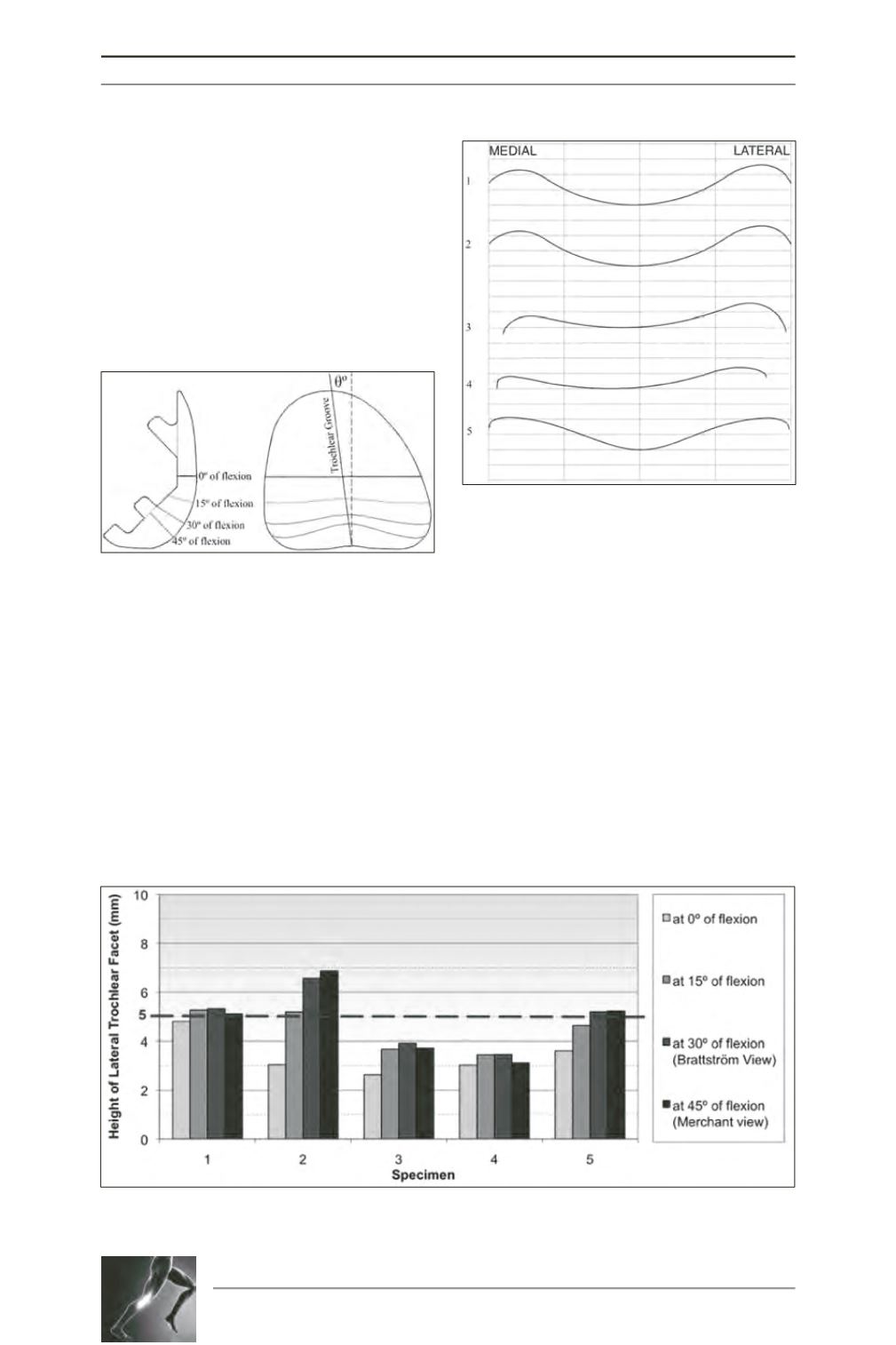
angle above 144º in the “Merchant view” or
above 143º in the “Brattström view” [20, 25,
22] and (
ii
) height of lateral trochlear facet less
than 5mm [20, 25, 24]. The coordinates of the
trochlear grooves were used to calculate a
linear regression (using the method of least
squares) in the frontal plane, and the trochlear
groove orientation was calculated from the
cosine of its gradient (fig. 3).
Results
The two-dimensional trochlear profiles at 30°
of flexion for all 5 implants are presented to
enable direct visual comparisons (fig. 4).
The sulcus angles of all trochlear profiles are
presented graphically (fig. 5). Four specimens
had a sulcus angle greater than 144° in the
“Merchant view” (45° of flexion), and thus all
but one specimen satisfied this first definition
of trochlear dysplasia. Five specimens had a
sulcus angle greater than 143° in the “Brattström
view” (30° of flexion), and thus all specimens
met the second definition of trochlear dysplasia.
We observed different sulcus angle progressions
in the range of flexion (0° to 45°): a considerable
decrease (>10º) in 2 specimens, and a negligible
decrease (<5º) in 3 specimens.
Fig. 3: Visual representation of trochlear profiles
measured: (a) trochlear profiles viewed in the
sagittal plane and (b) trochlear profiles viewed in
the frontal plane and trochlear groove orientation.
Fig. 4: Trochlear profiles of all specimens at 30° of
flexion.
Fig. 5: Sulcus angle for all specimens at different flexion angles. The dashed red line represents the
radiographic indicator of trochlear dysplasia (sulcus angle over 144º in the “Merchant view”).