








 56 / 242
56 / 242

M. Saffarini, P.G. Ntagiopoulos, G. Demey, B. Le Negaret, D. Dejour
56
designs are derived from the trochlear portions
of TKA models [12, 26, 11], we questioned
whether some PFA models also exhibit
characteristics of trochlear dysplasia. The
design of the trochlear compartment is arguably
more critical in PFA implants than in TKA
implants, because 78% of patients with isolated
patellofemoral arthritis also have pre-existent
trochlear dysplasia and patellar mal-tracking
[27] and therefore remain predisposed to
patellofemoral complications [7].
The purpose of this study was to quantify the
differences that exist between contemporary
PFA trochlear implants with specific attention
given to the sulcus angle and lateral facet height
at various degrees of knee flexion. The
hypothesis was that some of the designs would
meet the radiographic definition of trochlear
dysplasia and could explain some early
complications.
Because
patellofemoral
complications are usually caused by a
combination of factors related to surgical
technique and implant design, the authors did
not attempt to correlate the findings with
clinical results of the studied implants.
Materialand Methods
The authors formed a sample of 5 trochlear
components and identified and numbered each
specimen by its laser marking to determine its
manufacturer, model, serial number, size and
side The specimens included the following
models: Avon (Stryker, Mahwah, NJ), HLS
KneeTec (Tornier SA, Montbonnot, France),
Vanguard (Biomet Inc., Warsaw IN), PFC
(DePuy Orthopaedics Inc., Warsaw, IN),
NexGen (Zimmer Inc., Warsaw, IN) (
Table 1
).
Specimens were chosen based on their sizes
falling near the middlemost option of the
available range.
The specimens were each scanned using a
three-dimensional (3D) optical scanning
machine (ATOS II, GOM mbH, Braunschweig,
Germany). The coordinates of points scanned
on each specimen were rendered into smooth
surfaces using three-dimensional model
reconstruction software (Rapid Form, 3D
Systems Corp., South Carolina, USA), which
enabled full manipulation and measurement
using standard computer aided design software
(Pro/Engineer,
Parametric
Technology
Corporation, Massachusetts, USA).
The specimens were each oriented in a
consistent coordinate system, defined with the
“origin” at the tip of the most posterior fixation
peg and: (
i
) the ML axis parallel to the frontal
resection plane; (
ii
) the AP axis parallel to the
distal resection plane (or to its posterior tangent
in the case of a curved surface); (
iii
) the SI axis
orthogonal to the distal resection plane (or to
its posterior tangent in the case of a curved
surface). The three reference planes of each
specimen were hence defined: (
iv
) the ML and
SI axes for the frontal plane; (
v
) the AP and SI
axes for the sagittal plane; and (
vi
) the ML and
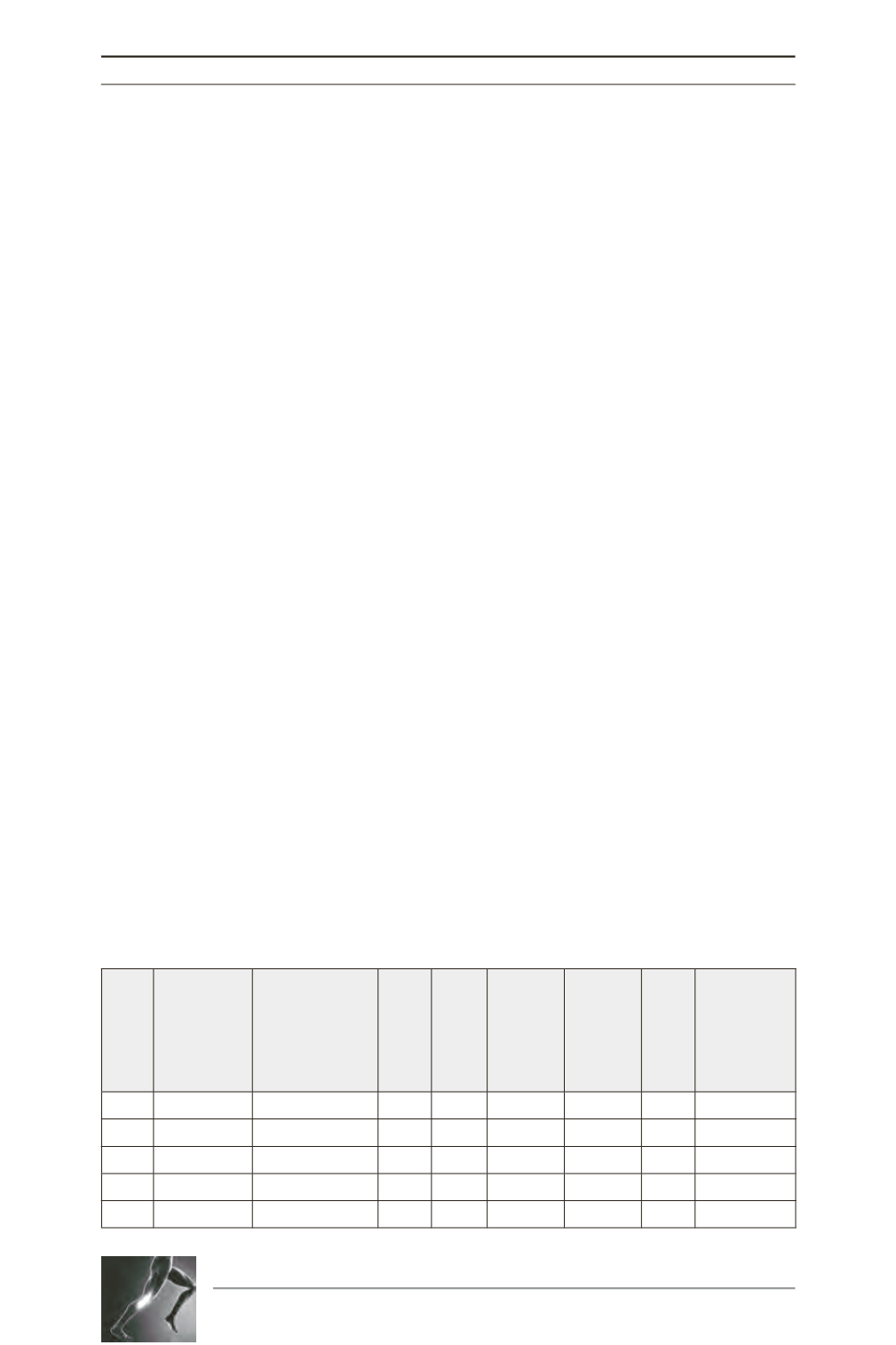
Table 1: List of the specimens measured and their principal dimensions.
Specimen
Manufacturer
Model
Size
Side
ML (mm)
AP (mm)
SI (mm)
Orientation of
Trochlear
Groove
1
Stryker
AvonTM M R 46.8
26.1 44.8
1.6º
2
Tornier
KneeTecTM 3
R 47.9
28.1 47.1
7.0º
3
Biomet
VanguardTM M L
46.3
38
53
2.0º
4
DePuy
PFC®
3
R 33.9
28.5 43.6 13.5º
5
Zimmer
NexGen® 3
R 45.1
24.5 42.9
7.3º