










 166 / 244
166 / 244

TIBIAL SLOPE AND ACL RUPTURE: MRI ASSESSMENT
165
DISCUSSION
Some studies found that the measurement of
posterior slope using lateral radiographs and
the measurement of meniscal insertion using
sagittal MRI images were both reproducible
and reliable [12], in contrast Han
et al.
[17]
declare that tibial slopes obtained from
conventional plain X-rays are of limited value
because they have poor reproducibility, caused
by tibial rotation in lateral view. The problem
inherent to the measurement of the tibial slope
on the short sagittal MRI sections of the knee is
the impossibility to adequately determine the
PTAA. To determine the PTAA, a section
covering a minimum of 150mm below the joint
gap of the knee is necessary [12].
The true tibial slope should be based on
measurements made at the center of the
articular regions of the medial and lateral
compartments of the tibial plateau.
The most important finding of the present study
was that the soft tissue tibial slope can be
measured reliably using an MRI-based method
where our results showed high ICC for all the
variants which reveal strong agreement
between the observers for all measurements.
It was hypothesized that patients with ACL
injury have larger tibial slope than normal
people and within the injured group, the lateral
tibial slope is larger than the medial one. The
results supported this hypothesis. Our results
are somehow similar to those observed by
Matsuda
et al.
[18], who reported a range of 5°
to 15.5° for medial tibial slope and a range of
0° to 14.5° for lateral tibial slope in their study
of subjects with normal knees.
Our results agreed with Brandon
et al.
[13]
who found that ACL-insufficient patients had a
significantly greater PTS than their negative
controls. In a resemble Studies, Todd
et al.
[19]
found that subjects in the noncontact ACL
group had significantly greater slope angles
than did control subjects. Stijak
et al.
[21]
found that the tibial slope on the lateral plateau
had a significantly higher value in the ACL
group than in the control group. The anterior
tibial translation during flexion was greater on
the lateral tibial plateau. This can explain why
the additional increase in the tibial slope
imparted stress on the ACL that could result in
its rupture.
The axial compression of a knee with a higher
LTS compared with MTS may cause greater
anterior motion of the lateral compartment of
the tibia compared with the medial one,
creating a net internal rotation of the tibia with
respect to the femur, which may increase
loading on the ACL [21]. Dejour and Bonnin
[24] demonstrated a mean 6mm increase in
anterior tibial translation (ATT) for each 10°
increase in posterior tibial slope in ACL-
deficient patients and healthy controls.
The effect of the posterior slope on knee
kinematics may be altered by the menisci.
Thus, the STS may reflect the true relationship
between the femoral & tibial condyles.
It was hypothesized that the soft tissues would
influence the slope in both compartments.
In contrast to the similar study of Lustig
et al.
[13] who declared that the menisci shift the
tibial slope towards the horizontal and the soft
tissue slope is more horizontal in the lateral
compartment of the knee compared to the
medial one, we found that the meniscal slope
was large in the injured group than the normal
and the soft tissue slope is more horizontal in
the lateral compartment of the knee compared
to the medial one.
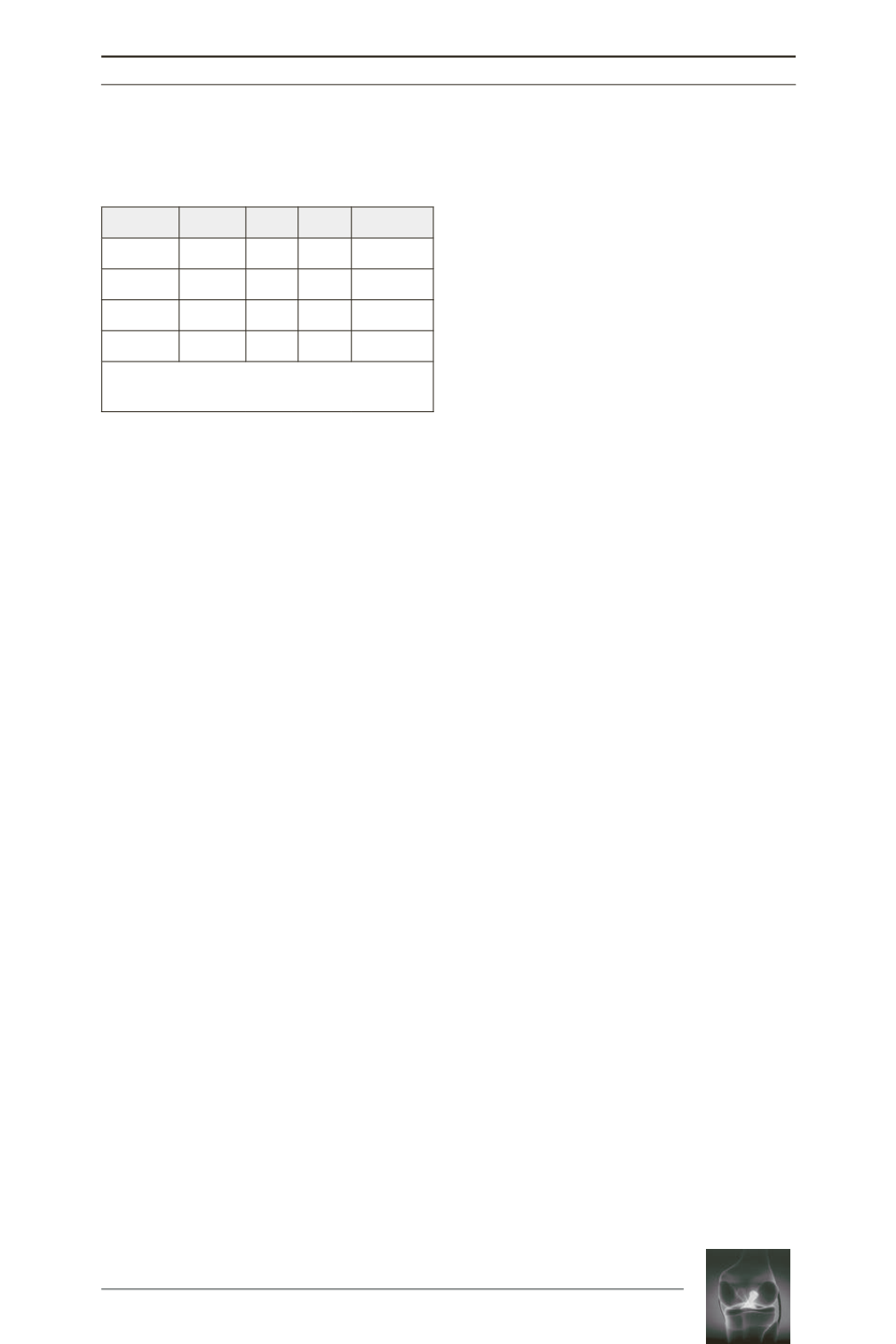
Table 4:
Represents the result of comparison of the
variants between examined and control groups
using independent student
t
-test:
Variants
t
-test
SD DOF
P
Value
LTS 6.76 3.30 198 0.0001
MTS 4.85 3.53 198 0.0001
LMS 5.67 4.80 198 0.0001
MMS 4.61 3.59 198 0.0001
SD:
standard deviation,
DOF:
degree of
freedom,
p
:
probability