










 22 / 324
22 / 324

throughout the whole rehabilitation period in
order to prevent inadequate mobilization and to
optimize leg muscle function. If toe-touch
weight-bearing is not possible, despite careful
preoperative instruction, or if poor compliance
is expected, the leg is placed in a continuous
passive- motion machine to maintain function
and to reduce postoperative swelling prior to
immobilization in a cylinder cast. Radiographs
are made on both the first postoperative day as
well as at eight weeks.
RESULTS
A correction of the intra-articular depression
and the valgus malalignment was achieved and
the anatomic lower-extremity axis was resto-
red in all 23 patients. The clinical results were
evaluated at a mean of thirteen years (range,
two to twenty-six years) after the reconstructi-
ve osteotomy. Two patients had an early failu-
re and were considered to have had a poor
result. Two other patients had severe progres-
sion of osteoarthritis after the osteotomy, four
had slight progression, and fifteen had no pro-
gression. There were no nonunions. There
were two superficial wound infections, which
were treated successfully without surgical
intervention. According to the scale of
Lysholm and Gillquist, the subjective result
was excellent for seventeen patients (74%),
good for three, fair for one, and poor for two.
COMBINED INTRA-ARTICULAR AND VARUS OPENING WEDGE OSTEOTOMY FOR LATERAL DEPRESSION…
21
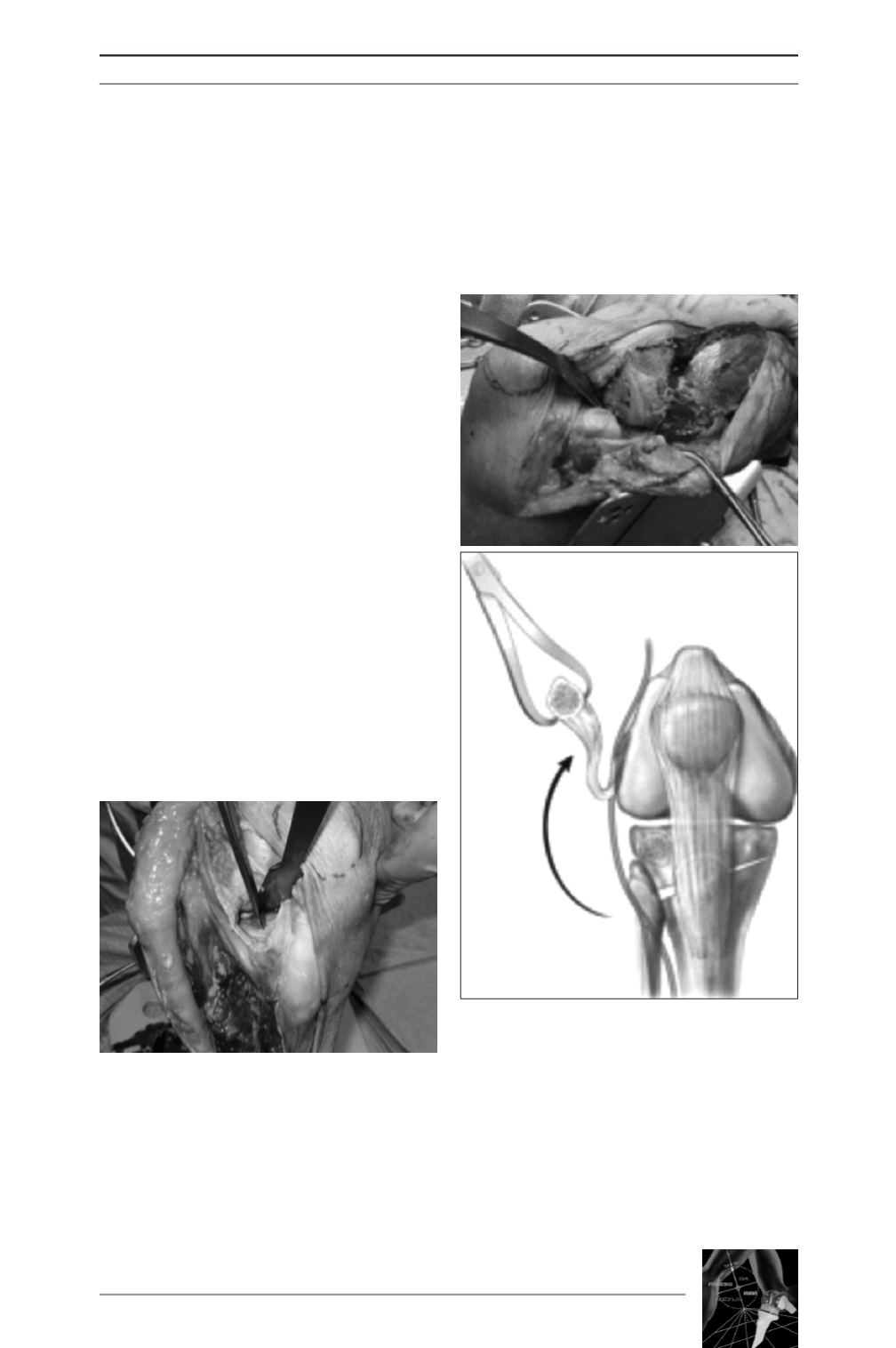
Fig. 2A, 2B: (Figs. Reprinted from: Kerkhoffs
GMMJ et al. J Bone Joint Surg Am. 2009; 91
Suppl: 101-1). After dissection of the per-
oneal nerve and the osteotomy of the Gerdy
tubercle as well as the fibular head, a full
exposure of the lateral tibial plateau can be
achieved. Eventually, the osteotomy of the
Gerdy tubercle can be fixed with the plate
used to secure the varus osteotomy of the
proximal part of the tibia, and the fibular
head osteotomy is routinely secured with a
3.5-mm lag screw.
Fig. 1: The exposure and intra-articular
osteotomy of the lateral tibial condyle is
done through a simple lateral arthrotomy.
(Reprinted, with permission, from: Marti RK,
Kerkhoffs GM. Osteotomies for malunions
of the tibial head. In: Marti RK, van
Heerwaarden RJ, editors. Osteotomies for
posttraumatic deformities. New York:
Thieme; 2008. p 479-94.)
A
B