










 264 / 324
264 / 324

TOTAL KNEE ARTHROPLASTY AFTER PRIOR KNEE ARTHROSCOPY
263
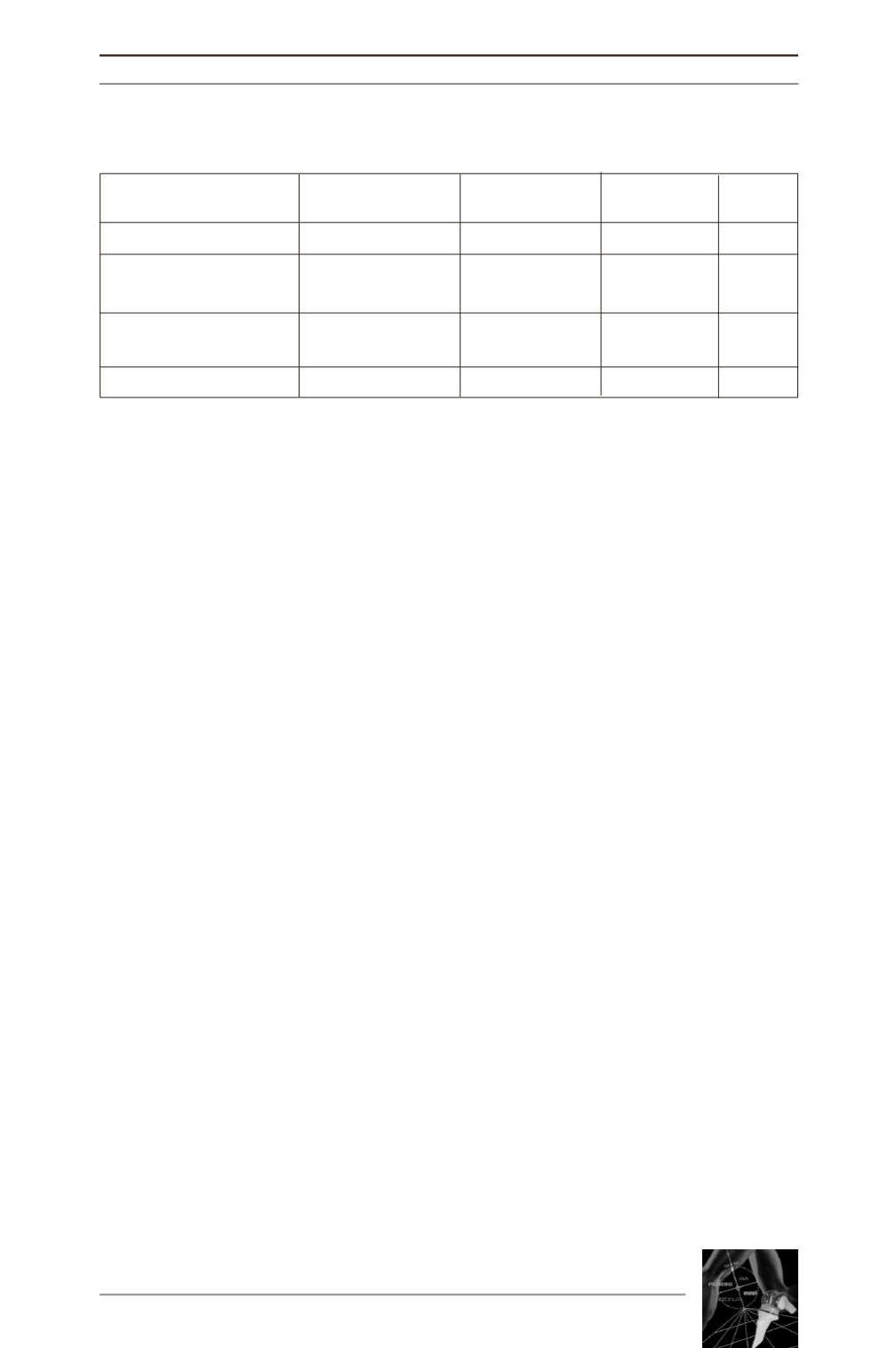
Group A
Group B
Group C *P value
(1119 patients )
(85 patients)
(146 patients)
Age (years)
72 (20 - 95)
71 (41-90)
69 (34-90)
<0.01
Sex
Female
854 (76%)
49 (58%)
91 (62%)
<0.001
Male
265 (24%)
36 (42%)
55 (38%)
<0.001
Side
Right
601 (54%)
47 (55%)
86 (59%)
NS
Left
518 (46%)
38 (45%)
60 (41%)
NS
BMI
29 (14.45-51.27)
29 (17.36-41.9) 27 (19.9-46.1)
=0.01
* NS non-significant statistical analysis between both study groups.
Table 1 : Characteristics of the study groups of patients (groups A, B and C)
At 120 months follow-up, the Kaplan-Meier
survival curves showed a survival rate of
98.1%, 90.9 and 94.8% of primary TKA sur-
vival rate for
group A, B and C
, respectively.
Post-operatively evaluation presented no dif-
ference in terms of improved IKS function
score, knee alignment, second surgical inter-
vention and revision TKA procedure.
However, group C showed lower IKS knee
score improvement (p=0.01), 11% of cases
were classified as moderate pain level
(p=0.01) and post-operative complication rate
was higher (22% of these cases) when compa-
red to other groups (p<0.001).
CONCLUSION
Our data confirms that prior knee surgery (bone
and soft tissue procedure) could be considered
a clinical condition that is predisposed to
higher postoperative complication and failures
rates in primary TKA (p<0.005 and p<0.001,
respectively) compared to the no prior surgery
group. Analyzing the three study groups, group
C showed A higher rate of postoperative com-
plications (p<0.001) and lower IKS knee
scores (p=0.01). However, statistical analysis
did not reveal a direct correlation between type
of prior knee surgery and TKA failures.
REFERENCES
GANDHI R, DE BEER J, LEONE J, PETRUCCELLI D,
WINEMAKER M, ADILI A. Predictive risk factors for stiff
knees in total knee arthroplasty.
J Arthroplasty (2006)
21(1): 46-52.
JEROSCH J, ALDAWOUDYAM. Arthroscopic treatment of
patients with moderate arthrofibrosis after total knee replace-
ment.
Knee Surg Traumatol Arthrosc (2007) 15(1): 71-7.
KLINGERHM, BAUMSMH, SPAHNG, ERNSTBERGERT.
A study of effectiveness of knee arthroplasty after arthro-
plasty.
Arthroplasty (2005) 21(6): 731-8.
McGINLEY BJ, CUSHNER FD, SCOTTWN. Debridement
arthroscopy. 10 year follow-up.
Clin Orthop Relat Res
(1999) 367: 190-4.
PIEDADE SR, PINAROLI A, SERVIEN E, NEYRET P. Is
previous knee arthroscopy related to worse results in prima-
ry total knee arthroplasty? Knee Surgery, Sports
Traumatology,
Arthroscopy, v. 17, p. 328-33, 2009.
PIEDADE SR, PINAROLI A, SERVIEN E, NEYRET P.
Revision after early aseptic failures in primary total knee
arthroplasty.
Knee Surgery, Sports Traumatology,
Arthroscopy, v. 17, p. 248-53, 2009.
PINAROLI A, PIEDADE SR, SERVIEN E, NEYRET P.
Intraoperative fractures and ligament tears during total knee
arthroplasty. A 1795 posterostabilized TKA continuous
series.
Revue de Chirurgie Orthopedique et Reparatrice de
l’Appareil Moteur, v. 95, p. 183-9, 2009.
PIEDADE SR, PINAROLI A, SERVIEN E, NEYRET P.
Tibial tubercle osteotomy in primary total knee arthrospla-
ty: a safe procedure or not?
Knee (Oxford), v. 15, p. 439-
46, 2008.
NELSON CL, SALEH KJ, KASSIM RA, WINDSOR R,
HAAS S, LASKIN R, SCULCO T. Total knee arthroplasty
after varus osteotomy of the distal part of the femur.
J Bone
Joint Surg Am (2003) 85(6): 1062-5.
PAPADOPOULOS EC, PARVIZI J, LAI CH, LEWALLEN
DG. Total knee arthroplasty following prior distal femoral
fracture.
Knee (2002) 9(4): 267-74.
PARVIZI J, HANSEN AD, SPANGEHL MJ. Total knee
arthroplasty following proximal tibial osteotomy: risk fac-
tors for failure.
J Bone Joint Surg Am (2004) 86(3): 474-9.
YANG SS, NISONSON B.Arthrosocpy surgery of the knee in
the geriatric patient.
Clin Orthop Relat Res (1995) 316: 50-8.