










 172 / 460
172 / 460

The history of the trochlear dysplasia in patella dislocation
171
It took almost 50 years, for a more meticulous
study on the anatomic characteristics of the
patients with instability by H. Brattström, a
paediatric orthopaedist from Österliden in
Sweden with a strong interest in rheumatologic
conditions, who focused on the reduced height
of the lateral trochlear facet in children. He was
the first to publish, in 1964, a study on trochlear
dysplasia on axial knee X-rays at 30° of flexion
and described it as a flattening of the trochlear
groove [27]. This was the first large-scale study
on the anatomy of the trochlea, the depth of the
groove and the height of the lateral facet was
described in patients with patellar dislocation,
but without notion of pathologic threshold
value. He discovered three types of trochlear
dysplasia:
1)
hypoplasia of the medial femoral
condyle which is the most frequent type,
2)
aplasia of the medial condyle and
3)
total dysplasia of both condyles
with a flat or convex distal femoral
trochlea. At that time, there was a
growing interest in many
European centers, where surgeons
believed that the flattened
trochlear groove was a major
factor in patellar dislocation [10].
Then, a more drastic concept of
surgically correcting the dysplasia
was proposed by a french surgeon
from Paris Y. Masse in 1978, who
focused on a technique to remodel
the trochlea without injuring its
cartilage [28] in which the goal
was to remove the posterior part
of the trochlea and then push it
posteriorly with an impactor, but with no
consideration on the medial or lateral facet.
It wasn’t until 1985, that the Belgians
radiologists B. Maldague and J. Malghem
focused on the study of trochlea
“and its
dysplasias”
in lateral X-rays [29, 30]. They
described an anomaly that could be either
generalized or focal to the proximal trochlea
and they correlated an increased sulcus angle
of more than 145° with trochlear dysplasia.
They measured the proximal trochlear depth
1cm below the upper limit of the trochlear
groove in lateral X-rays and found that it was
on average 2.7 mm in patients with patellar
dislocation, in contrast to 5.9 mm in the
asymptomatic group.
Until that time, trochlear dysplasia was a
pathologic radiographic finding in patients with
patellar dislocation. Although how strongly
trochlear dysplasia was correlated in the clinical
setting with patellar dislocation not only to the
paediatric population was not yet documented,
the interest on trochlear dysplasia was emerging
in the university hospital of Lyon during the
1980’s with a series of publications by Henri
Dejour and Gilles Walch, who presented some
of the most essential and classic data on patellar
instability (fig. 2). They were the first to link
the occurrence of trochlear dysplasia in patients
with patellar dislocation and in asymptomatic
controls. They used their 1984 classification of
Fig. 1: The lateral facet elevating trochleoplasty
proposed by Albee.
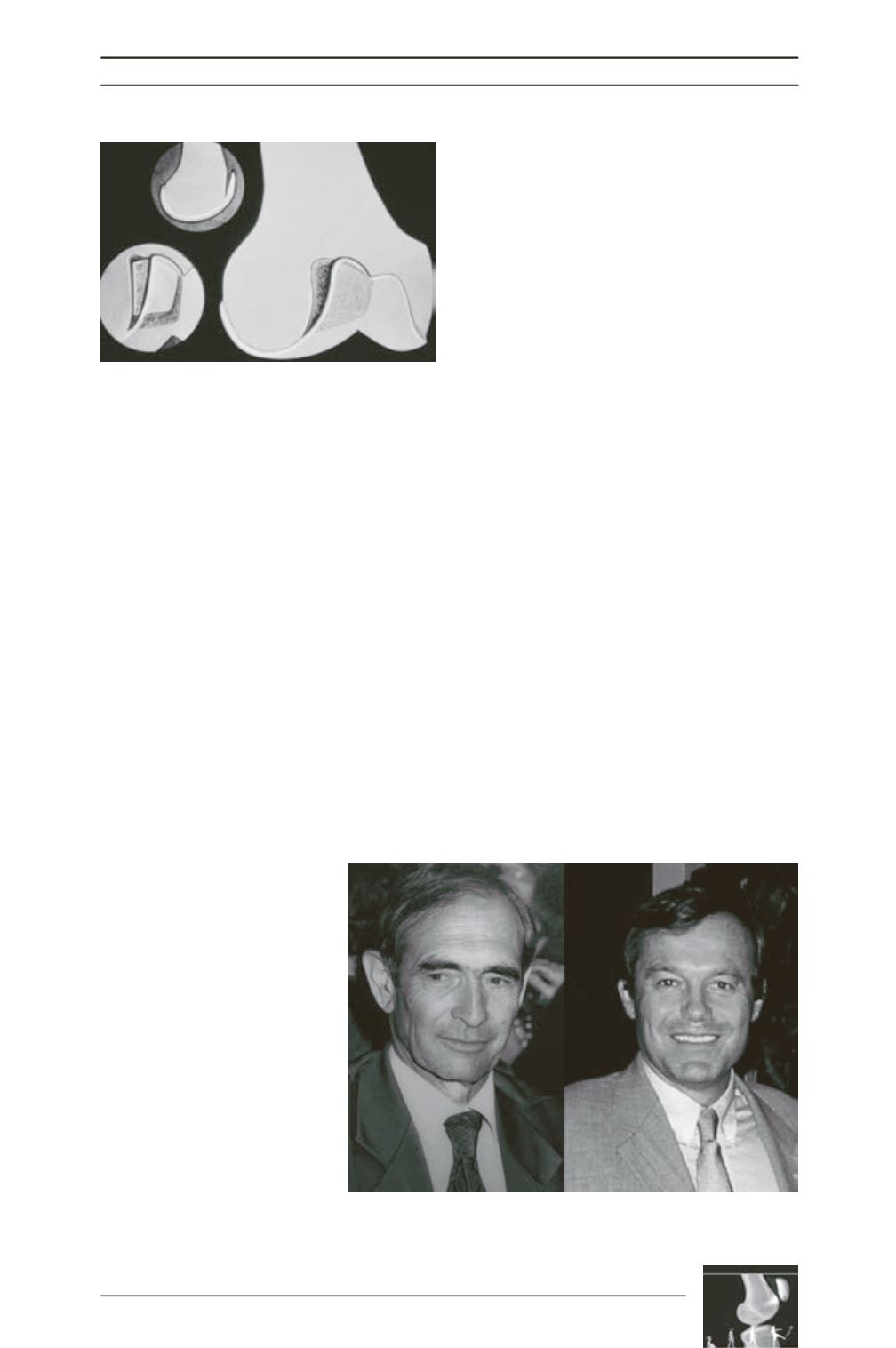
Fig. 2: Henri Dejour (left) and Gilles Walch pioneers in the field of
patellofemoral disorders during the 1980’s.