










 173 / 460
173 / 460

D. Dejour, P.G. Ntagiopoulos
172
permanent, habitual, and recurrent patellar
dislocation, in which they started performing
X-ray measurement of the trochlea and its
position related to the anterior femoral cortex.
It is worth mentioning that at the time, surgeons
in Lyon were already using true lateral X-rays
for a different method developed for measuring
anterior tibial translation in ACL ruptures.
They introduced the “crossing sign”, which
became the pathognomonic sign for trochlear
dysplasia on lateral X-rays (fig. 3).
This fundamental work on the definition of
trochlear dysplasia and on its consistent
presence in patients with patellar dislocation
was presented and published in 1987 during the
6
th
edition of the meeting
“Les Journées
Lyonnaises de Chirurgie du Genou”
[12] and
was later issued in 1990 [31]. It was the result
of a huge effort from the whole “Lyon’s School”
of surgeons who studied the radiographic
findings in more than 1,800 patients and
presented their standardized approach on
patellofemoral instability that would be quoted
and followed widely in the future. H. Dejour
and G. Walch introduced the definition of
dysplasia as a shallow, flat or even convex
trochlear groove by using some of the
radiographicmethods of Raguet [32], Maldague
and Malghem [29, 30] and by examining true
lateral X-rays where the posterior femoral
condyles were
superimposed
[8]. They recorded
that trochlear dysplasia was present in 96% of
patients with documented patellar dislocation
and only in 3% of a control population, thus
presenting dysplasia as the
most consistent
anatomic abnormality underlying in patients
with patellofemoral instability
. Yet, the most
important attribution of this classic study was
the introduction of the first
quantitative and
qualitative
criteria of trochlear dysplasia.
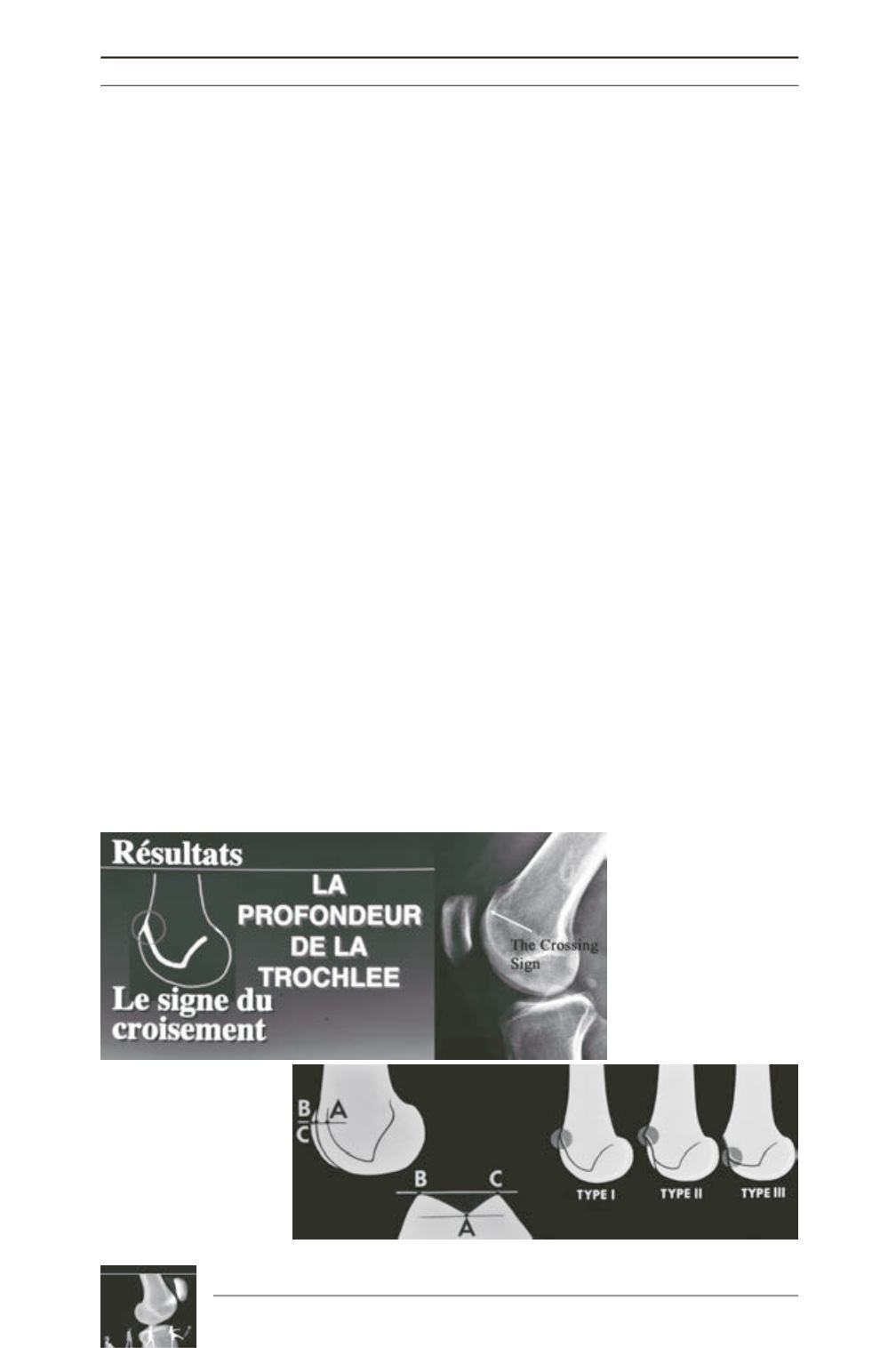
H. Dejour and G. Walch described the crossing
sign as a simple yet fundamental qualitative
factor of trochlear dysplasia. It represented the
point where the line of the trochlear floor
intersects the anterior contour of the lateral
femoral condyle and the level where the
trochlea is flat. The crossing sign could have
three different appearances in reference to the
level of the intersection (proximally or distally)
and the symmetry or not of the medial and
lateral femoral condyles (fig. 4). With these
data, the first classification of trochlear
dysplasia was introduced, which was focused
on how proximally or distally (on the flexion-
extension arc of the knee) the trochlea becomes
dysplastic:
Type I
corresponds to minor
dysplasia where the trochlea is flat at only one
point in its superior (proximal) portion and the
condyles are symmetrical,
Type II
has separate
Fig. 3: (Original slide) The
introductionofthe ‘crossing
sign’ as pathognomonic
sign and qualitative factor
for trochlear dysplasia.
Fig. 4: The crossing sign
had 3 different types in
reference to the level of the
intersection (proximally or
distally) and the symmetry
or not of the medial and
lateral femoral condyles.